

Review
doi: 10.1186/1476-7120-8-7.
Echocardiography in patients with hypertrophic cardiomyopathy: usefulness of old and new techniques in the diagnosis and pathophysiological assessment
Affiliations
- PMID: 20236538
- PMCID: PMC2848131
- DOI: 10.1186/1476-7120-8-7
Item in Clipboard
Review
Echocardiography in patients with hypertrophic cardiomyopathy: usefulness of old and new techniques in the diagnosis and pathophysiological assessment
Cardiovasc Ultrasound.
.
Abstract
Hypertrophic cardiomyopathy (HCM) is one of the most common inherited cardiomyopathy. The identification of patients with HCM is sometimes still a challenge. Moreover, the pathophysiology of the disease is complex because of left ventricular hyper-contractile state, diastolic dysfunction, ischemia and obstruction which can be coexistent in the same patient. In this review, we discuss the current and emerging echocardiographic methodology that can help physicians in the correct diagnostic and pathophysiological assessment of patients with HCM.
Figures
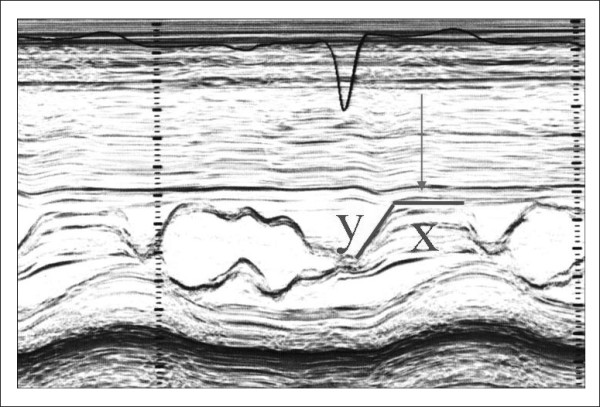
Systolic anterior motion (SAM) of the mitral valve visualized by M-Mode echocardiography. X represent the duration of SAM, whereas Y represent the time elapsed between the beginning of SAM and the SAM-septal contact (see text for more details).
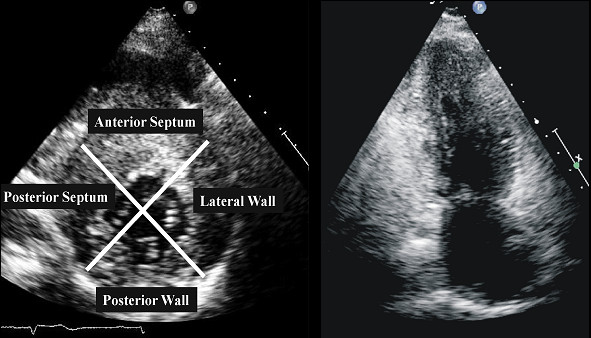
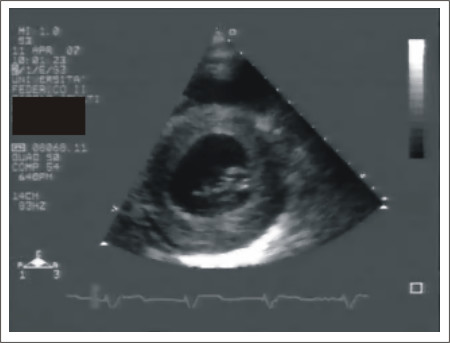
Left ventricular walls dived in four regions in a patients with HCM. Right panel. Apical view in a patient with apical hypertrophy.
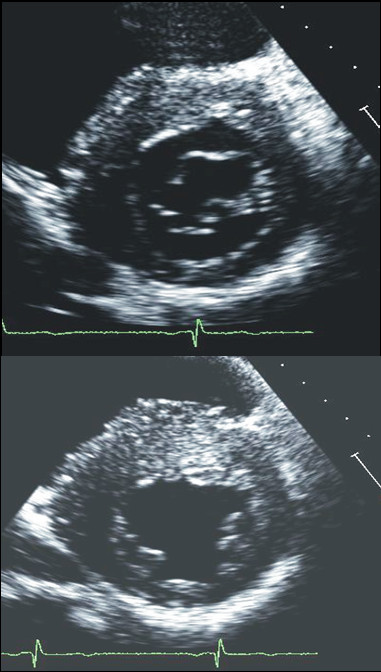
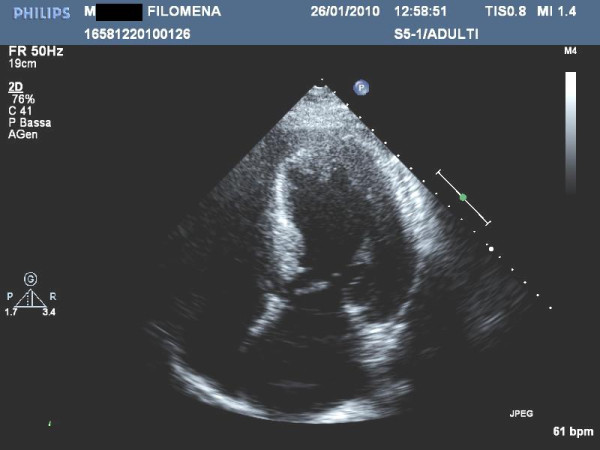
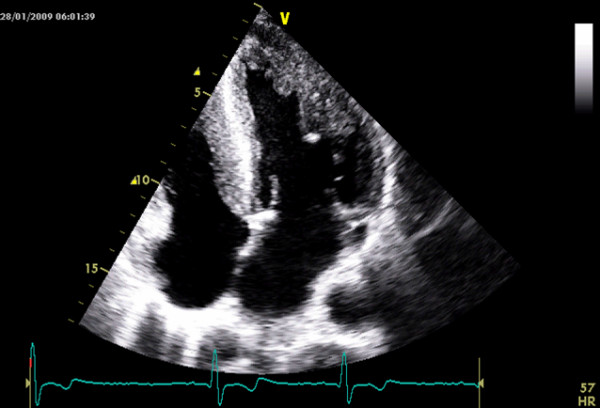
Examples of patients with hypertrophic cardiomyopathy with typical asymmetrical left ventricular hypertrophy.
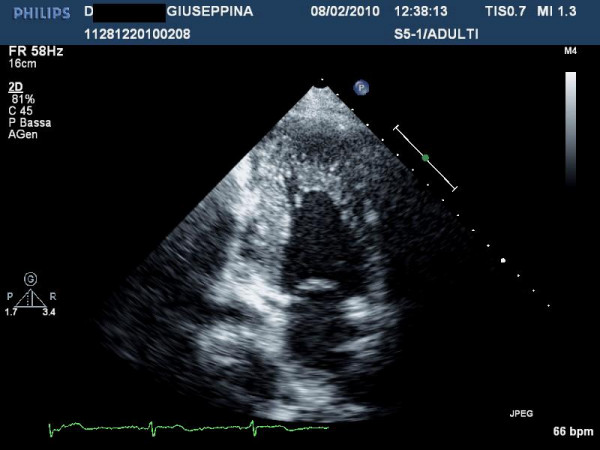
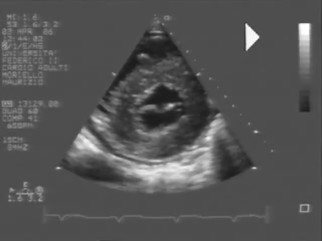
Patient with left ventricular non compaction. This patient was sottoposed to echocardiography in the contest of family screening for apical hypertrophic cardiomyopathy.
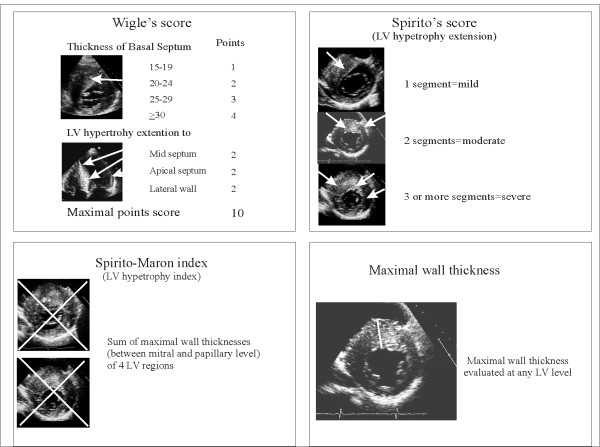
Echocardiographic methods to identify the degree and the extension of left ventricular hypertrophy in patients with hypertrophic cardiomyopathy. LV = left ventricular
Patient with end stage hypertrophic cardiomyopathy: note the absence of thinning: the left ventricular ejection fraction is 40%.

Patient with extreme left ventricular symmetrical hypertrophy. At electrocardiography patient showed a short PR. The patient was referred for aminotransferase and creatinine phosphokinase dosage and for genetic testing.
Young male with definitive diagnosis of Anderson- Fabry disease. For courtesy of Dr L. Spinelli.
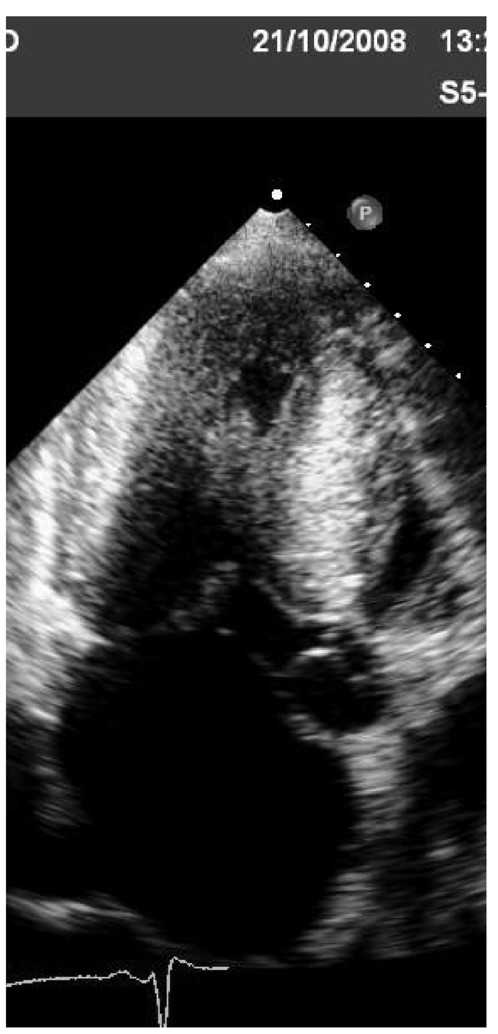
Patient with definite diagnosis of mithocondropathy done by neurologists. Echocardiography shows mild symmetric hypertrophy with mild reduction of left ventricular ejection fraction. During follow-up patient developed severe grade of AV block needing pace-maker and severe reduction of ejection fraction needing resynchronization.
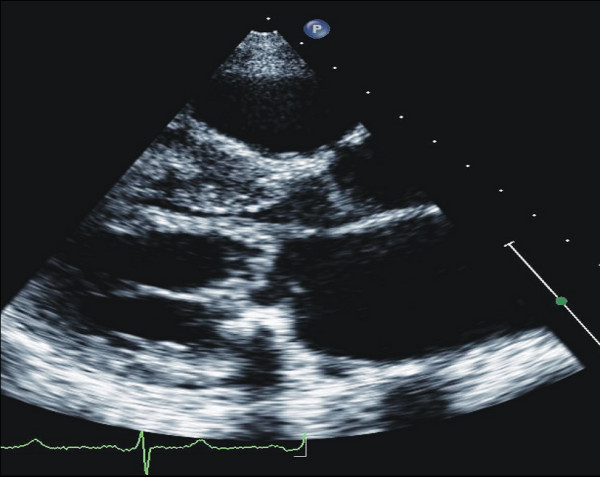
Patient with definitive diagnosis of amyloidosis. Note the pericardial effusion.
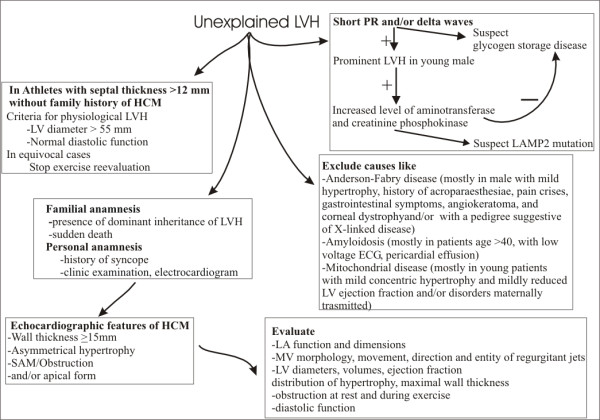
Scheme for the clinical and echocardiographic approach in patients with unexplained left ventricular hypertrophy. LV = left ventricular
Mid ventricular obstruction with an hourglass appearance.
Example of patients with abnormal direct insertion of papillary muscles into anterior mitral leaflet.
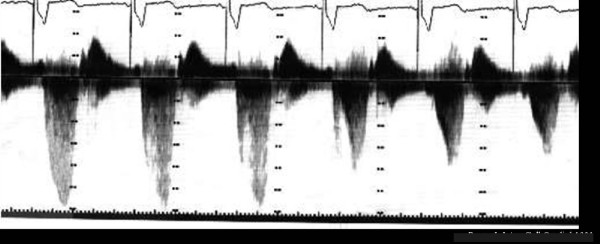
Differentiation between mitral regurgitation (first cardiac cycles) and left ventricular outflow tract gradient (last cardiac cycles). This was obtained by orienting the probe more medially and anteriorly.
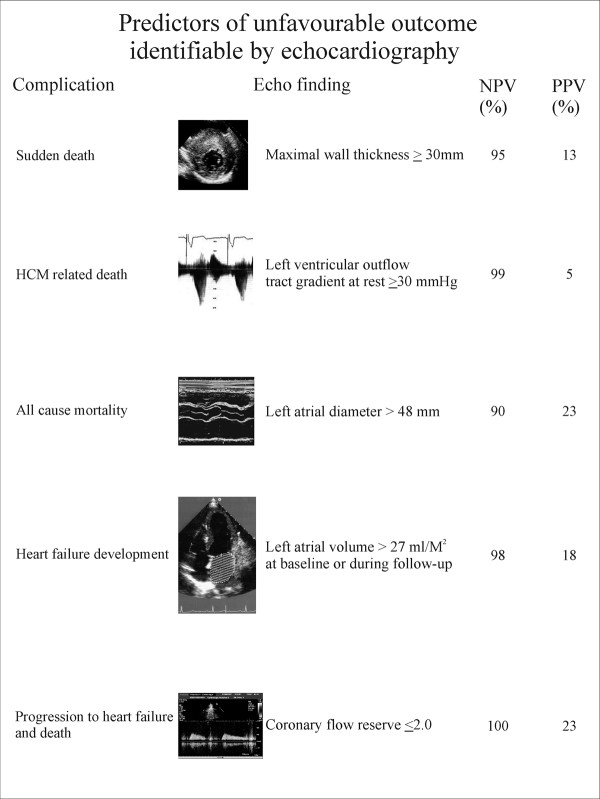
Echocardiographic findings and their prognostic impact in patients with HCM.
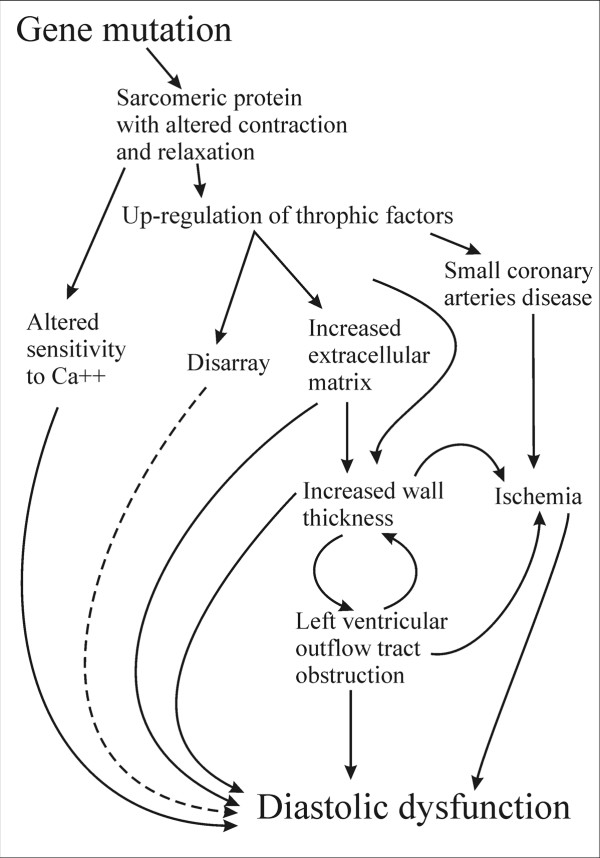
Mechanisms linked to diastolic dysfunction in patients with hypertrophic cardiomyopathy. Dashed lines represent links not yet well demonstrated.
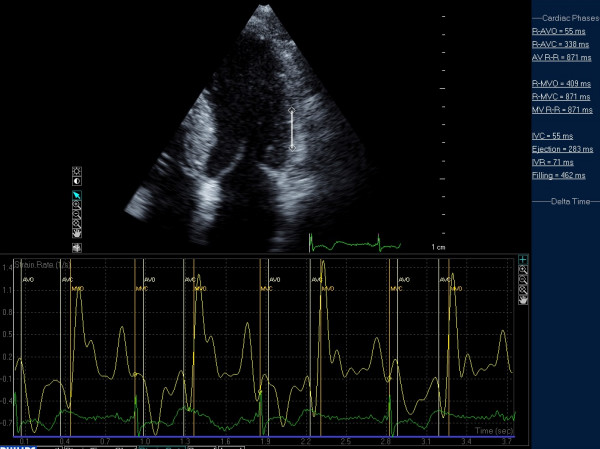
Example of post-systolic strain in a patient with HCM.
Similar articles
-
Echocardiography in hypertrophic cardiomyopathy: the role of conventional and emerging technologies.JACC Cardiovasc Imaging. 2008 Nov;1(6):787-800. doi: 10.1016/j.jcmg.2008.09.002. Epub 2008 Nov 18. JACC Cardiovasc Imaging. 2008. PMID: 19356516 Review.
-
Echocardiography in hypertrophic cardiomyopathy diagnosis, prognosis, and role in management.Eur J Echocardiogr. 2009 Dec;10(8):iii9-14. doi: 10.1093/ejechocard/jep157. Eur J Echocardiogr. 2009. PMID: 19889657 Review.
-
[Role of Doppler echocardiography in the diagnostics and therapy of hypertrophic cardiomyopathy].Cas Lek Cesk. 2006;145(4):279-83. Cas Lek Cesk. 2006. PMID: 16639927 Review. Czech.
-
Vector flow mapping in obstructive hypertrophic cardiomyopathy to assess the relationship of early systolic left ventricular flow and the mitral valve.J Am Coll Cardiol. 2014 Nov 11;64(19):1984-95. doi: 10.1016/j.jacc.2014.04.090. Epub 2014 Nov 3. J Am Coll Cardiol. 2014. PMID: 25440093
-
The role of echocardiography in hypertrophic cardiomyopathy.Curr Cardiol Rep. 2015 Feb;17(2):6. doi: 10.1007/s11886-014-0560-x. Curr Cardiol Rep. 2015. PMID: 25618305 Review.
Cited by
-
Myocardial Strain and Association With Clinical Outcomes in Danon Disease: A Model for Monitoring Progression of Genetic Cardiomyopathies.J Am Heart Assoc. 2021 Dec 7;10(23):e022544. doi: 10.1161/JAHA.121.022544. Epub 2021 Nov 30. J Am Heart Assoc. 2021. PMID: 34845930 Free PMC article.
-
Efficacy of echocardiography for differential diagnosis of left ventricular hypertrophy: special focus on speckle-tracking longitudinal strain.J Echocardiogr. 2021 Jun;19(2):71-79. doi: 10.1007/s12574-020-00508-3. Epub 2021 Jan 18. J Echocardiogr. 2021. PMID: 33460030 Free PMC article. Review.
-
Global longitudinal strain in pre-symptomatic patients with mutation for transthyretin amyloidosis.Orphanet J Rare Dis. 2024 Dec 5;19(1):458. doi: 10.1186/s13023-024-03473-7. Orphanet J Rare Dis. 2024. PMID: 39639351 Free PMC article.
-
A longitudinal study on BIO14.6 hamsters with dilated cardiomyopathy: micro-echocardiographic evaluation.Cardiovasc Ultrasound. 2011 Dec 8;9:39. doi: 10.1186/1476-7120-9-39. Cardiovasc Ultrasound. 2011. PMID: 22151912 Free PMC article.
-
Longitudinal strain bull's eye plot patterns in patients with cardiomyopathy and concentric left ventricular hypertrophy.Eur J Med Res. 2016 May 10;21(1):21. doi: 10.1186/s40001-016-0216-y. Eur J Med Res. 2016. PMID: 27165726 Free PMC article. Review.
References
-
- Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH, Spirito P, Ten Cate FJ, Wigle ED. ACC/ESC clinical expert consensus document on hypertrophic cardiomyopathy: a report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines (Committee to Develop an Expert Consensus Document on Hypertrophic Cardiomyopathy) J Am Coll Cardiol. 2003;42:1687–713. doi: 10.1016/S0735-1097(03)00941-0. - DOI - PubMed
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, Dubourg O, Kühl U, Maisch B, McKenna WJ, Monserrat L, Pankuweit S, Rapezzi C, Seferovic P, Tavazzi L, Keren A. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270–6. doi: 10.1093/eurheartj/ehm342. - DOI - PubMed
-
- Doi YL, McKenna WJ, Oakley CM, Goodwin JF. 'Pseudo' systolic anterior motion in patients with hypertensive heart disease. Eur Heart J. 1983;4:838–45. - PubMed
-
- Pollick C, Rakowski H, Wigle ED. Muscular subaortic stenosis: the quantitative relationship between systolic anterior motion and the pressure gradient. Circulation. 1984;69:43–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
