

Myocardial effects of VDR activators in renal failure
- PMID: 20236614
- PMCID: PMC2906634
- DOI: 10.1016/j.jsbmb.2010.03.026
Myocardial effects of VDR activators in renal failure
Abstract
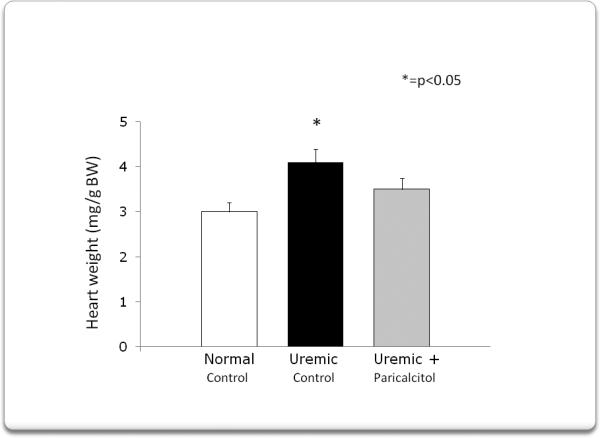
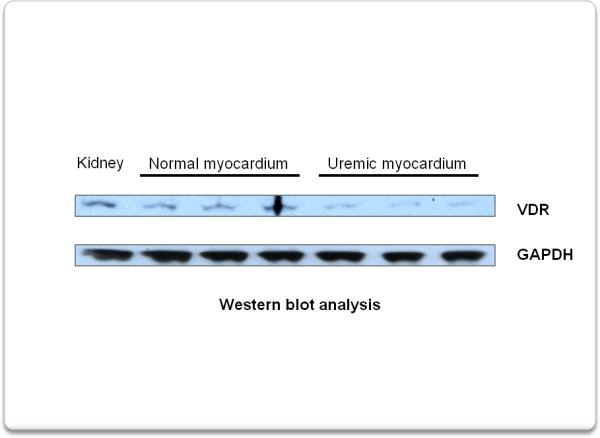
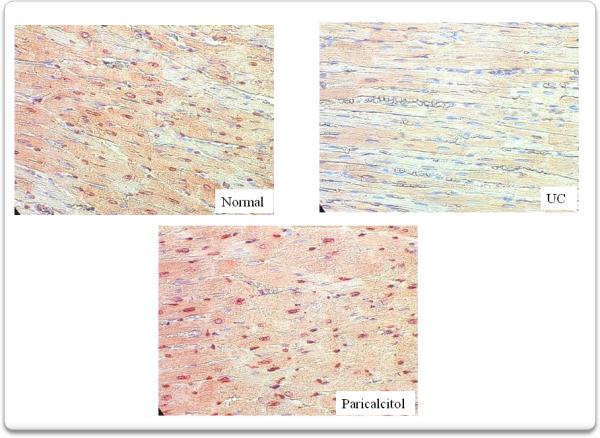
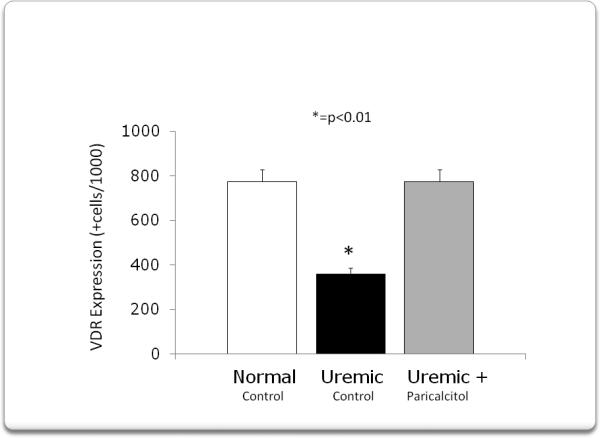
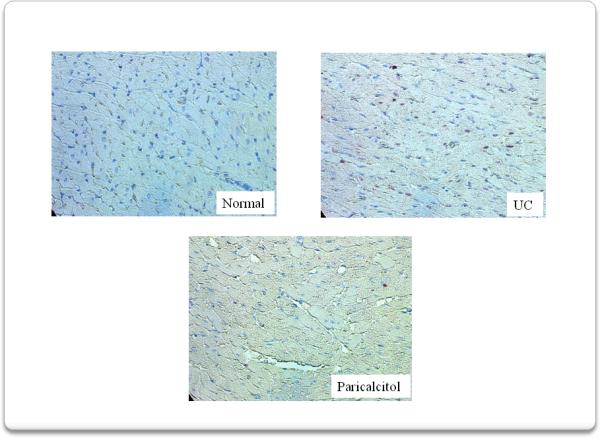
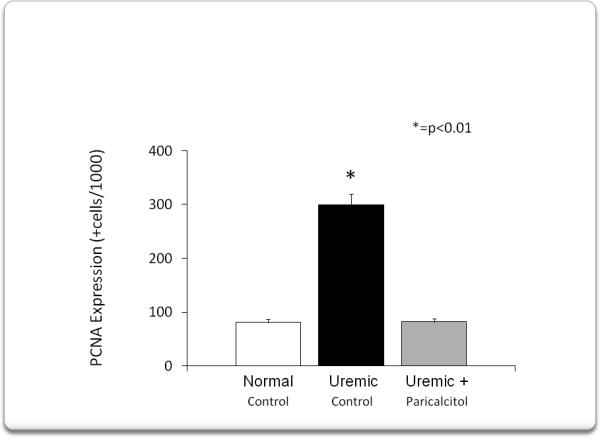
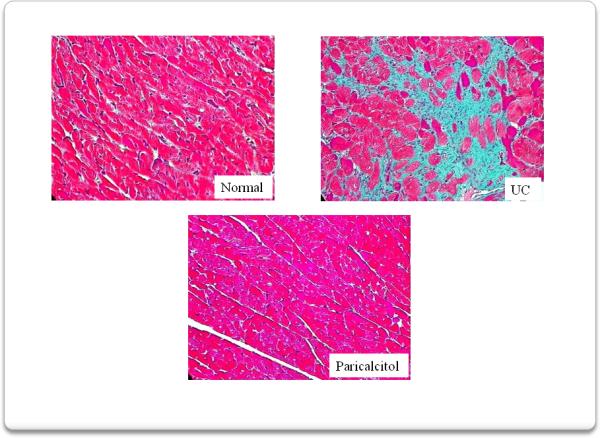
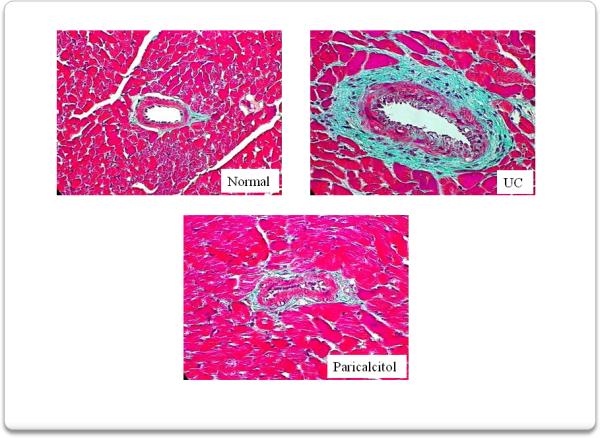
Cardiovascular complications are the leading cause of death in patients with chronic kidney disease (CKD). Traditional causes such as diabetes, smoking, aging and hypertension do not fully explain the high rate of morbidity from cardiovascular disease seen in these patients. The renin-angiotensin-aldosterone system (RAAS) regulates extracellular volume homeostasis, which contributes to blood pressure stability. Overactivity of this system is involved in the pathophysiology of cardio-renal disease. New evidence suggests that vitamin D receptor activators (VDRAs) have a suppressive effect on the RAAS; however, VDRAs also have anti-inflammatory and anti-fibrotic effects. We have demonstrated that paricalcitol, a VDRA, ameliorates left ventricular hypertrophy (LVH) in uremic rats by up-regulating the VDR, decreasing myocardial PCNA and also decreasing myocardial oxidative stress. Thus, paricalcitol can suppress the progression of LVH, myocardial and perivascular fibrosis and myocardial arterial vessel thickness presumably by up-regulating the VDR. Paricalcitol may prove to have a substantial beneficial effect on cardiac disease and its outcome in patients with CKD. Prospective randomized studies in CKD patients are necessary to confirm these results.
Copyright (c) 2010 Elsevier Ltd. All rights reserved.
Figures
References
-
- Teng M, Wolf M, Lowrie E, et al. Survival of patients undergoing hemodialysis with paricalcitol or calcitriol therapy. N Engl J Med. 2003;349:446–56. - PubMed
-
- Teng M, Wolf M, Ofsthun MN, et al. Activated injectable vitamin D and hemodialysis survival: a historical cohort study. J Am Soc Nephrol. 2005;16:1115–25. - PubMed
-
- Kalantar-Zadeh K, Kuwaen, Regidor D, et al. Survival predictability time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006;70:771–780. - PubMed
-
- Tentori F, Hunt WC, Stidley CA, et al. Mortality risk among hemodialysis patients receiving different vitamin D analogs. Kidney Int. 2006;70:1858–65. - PubMed
-
- Dusso A, Brown AJ. Slatopolsky E: Vitamin D. Am J Physiol- Renal Physiol. 2005;289:8028.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
