

Thymus transplantation
- PMID: 20236866
- PMCID: PMC3646264
- DOI: 10.1016/j.clim.2010.02.007
Thymus transplantation
Abstract
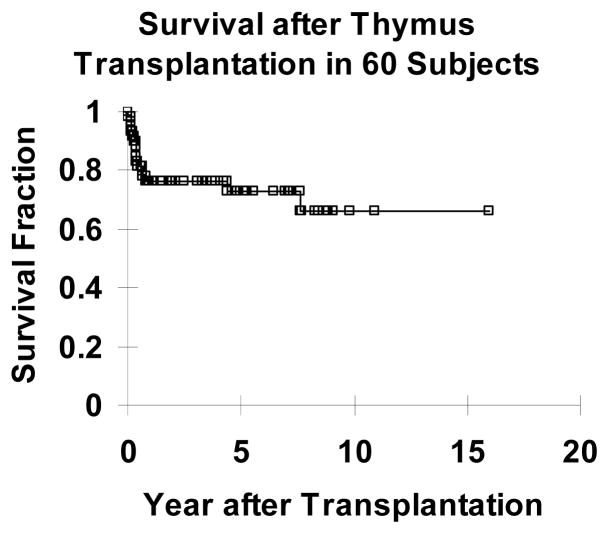
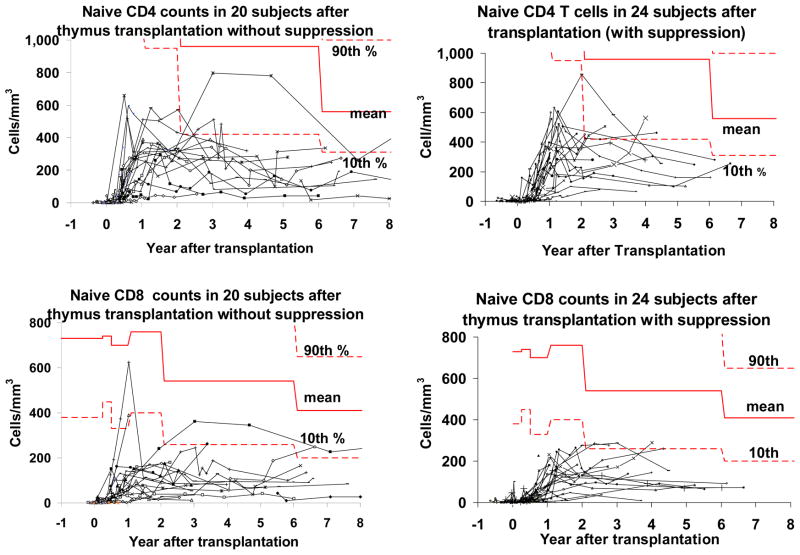
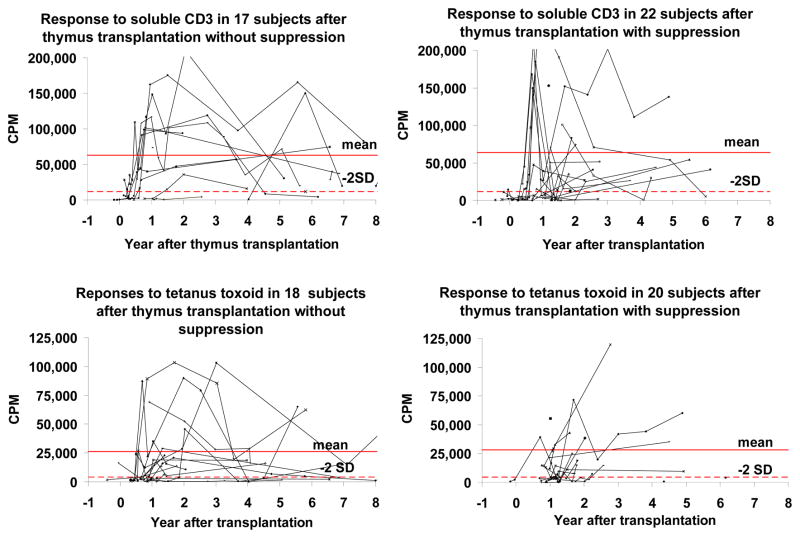
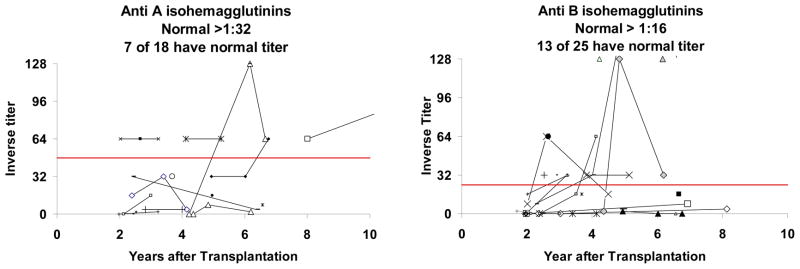
Thymus transplantation is a promising investigational therapy for infants born with no thymus. Because of the athymia, these infants lack T cell development and have a severe primary immunodeficiency. Although thymic hypoplasia or aplasia is characteristic of DiGeorge anomaly, in "complete" DiGeorge anomaly, there is no detectable thymus as determined by the absence of naive (CD45RA(+), CD62L(+)) T cells. Transplantation of postnatal allogeneic cultured thymus tissue was performed in sixty subjects with complete DiGeorge anomaly who were under the age of 2 years. Recipient survival was over 70%. Naive T cells developed 3-5 months after transplantation. The graft recipients were able to discontinue antibiotic prophylaxis, and immunoglobulin replacement. Immunosuppression was used in a subset of subjects but was discontinued when naive T cells developed. The adverse events have been acceptable with thyroid disease being the most common. Research continues on mechanisms underlying immune reconstitution after thymus transplantation.
Copyright 2010 Elsevier Inc. All rights reserved.
Figures
References
-
- Markert ML, Devlin BD. Thymic reconstitution. In: Rich RR, Fleischer SW, Schroeder T, Weyand HW, Frew CM, editors. A Clinical Immunology. 3. Edinburgh: Elsevier; 2008. pp. 1253–62.
-
- Markert MLDB, McCarthy EA, Chinn IK, Hale LP. Thymus Transplantation. In: Lavinin CMC, Morandi U, Schoenhuber R, editors. Thymus Gland Pathology: Clinical, Diagnostic, and Therapeutic Features. Milan, Springer-Verlag; Italia: 2008. pp. 255–67.
-
- Rice HE, Skinner MA, Mahaffey SM, Oldham KT, Ing RJ, Hale LP, et al. Thymic transplantation for complete DiGeorge syndrome: medical and surgical considerations. J Pediatr Surg. 2004 Nov;39(11):1607–15. - PubMed
-
- Markert ML, Li J, Devlin BH, Hoehner JC, Rice HE, Skinner MA, et al. Use of allograft biopsies to assess thymopoiesis after thymus transplantation. J Immunol. 2008 May 1;180(9):6354–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
