

Critically ill infants and children with influenza A (H1N1) in pediatric intensive care units in Argentina
- PMID: 20237757
- PMCID: PMC7095244
- DOI: 10.1007/s00134-010-1853-1
Critically ill infants and children with influenza A (H1N1) in pediatric intensive care units in Argentina
Abstract
Objective: To determine the epidemiological features, course, and outcomes of critically ill pediatric patients with Influenza A (H1N1) virus.
Design: Prospective cohort of children in pediatric intensive care units (PICUs) due to Influenza A (H1N1) virus infection.
Setting: Seventeen medical-surgical PICUs in tertiary care hospital in Argentina.
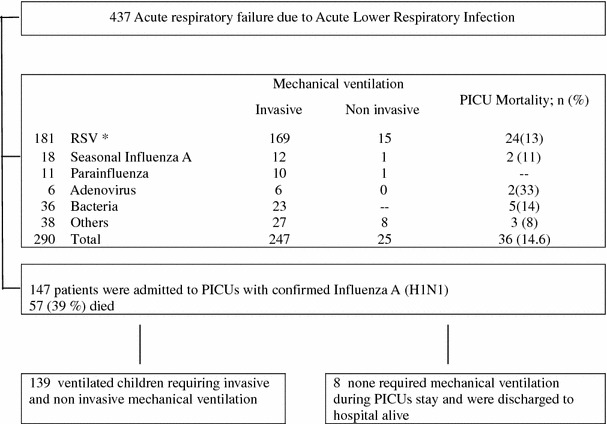
Patients: All consecutive patients admitted to the PICUs with influenza A (H1N1) viral infection from 15 June to 31 July 2009.
Measurements and main results: Of 437 patients with acute lower respiratory infection in PICUs, 147 (34%) were diagnosed with influenza A (H1N1) related to critical illness. The median age of these patients was 10 months (IQR 3-59). Invasive mechanical ventilation was used in 117 (84%) on admission. The rate of acute respiratory distress syndrome (ARDS) was 80% (118 of 147 patients). Initial non-invasive ventilation failed in 19 of 22 attempts (86%). Mortality at 28 days was 39% (n = 57). Chronic complex conditions (CCCs), acute renal dysfunction (ARD) and ratio PaO(2)/FiO(2) at day 3 on MV were independently associated with a higher risk of mortality. The odds ratio (OR) for CCCs was 3.06, (CI 95% 1.36-6.84); OR for ARD, 3.38, (CI 95% 1.45-10.33); OR for PaO(2)/FiO(2), 4 (CI 95% 1.57-9.59). The administration of oseltamivir within 24 h after admission had a protective effect: OR 0.2 (CI 95% 0.07-0.54).
Conclusions: In children with ARDS, H1N1 as an etiologic agent confers high mortality, and the presence of CCCs in such patients increases the risk of death.
Figures
References
-
- Ministerio de Salud de Argentina (2009) Influenza pandémica H1N1. http://municipios.msal.gov.ar/h1n1/parte_influenza/parte-65-fecha-05-08-...
-
- Monteverde E, Fernandez A, Farias JA. Segundo Estudio Internacional de la Ventilación Mecanica en Pediatría. Medicina Intensiva (Argentina) 2009;26:32.
-
- WHO (2009) Human infection with pandemic (H1N1) 2009 virus: updated interim WHO guidance on global surveillance. http://www.who.int/csr/disease/swineflu/WHO_case_definition_swine_flu_20...
-
- Slater A, Shann F, Pearson G. PIM2: a revised version of the Paediatric Index of Mortality. Intensive Care Med. 2003;29:278–285. - PubMed
-
- Feudtner C, Christakis DA, Connell FA. Pediatric deaths attributable to complex chronic conditions: a population-based study of Washington State, 1980–1997. Pediatrics. 2000;106:205–209. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
