

Complications associated with thoracic pedicle screws in spinal deformity
- PMID: 20237943
- PMCID: PMC2989291
- DOI: 10.1007/s00586-010-1316-y
Complications associated with thoracic pedicle screws in spinal deformity
Abstract
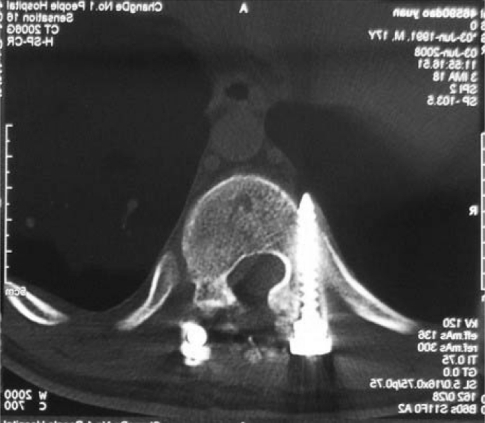
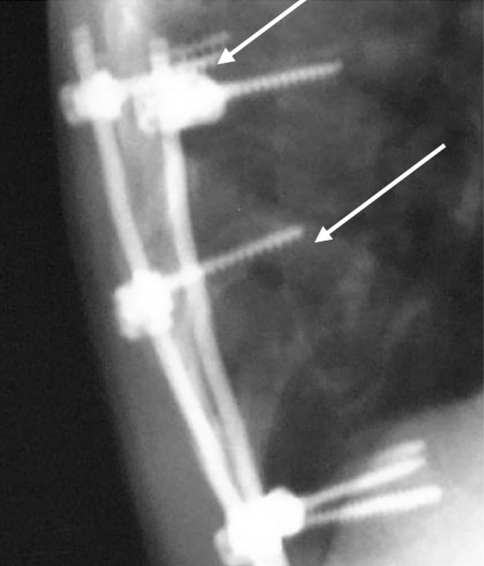
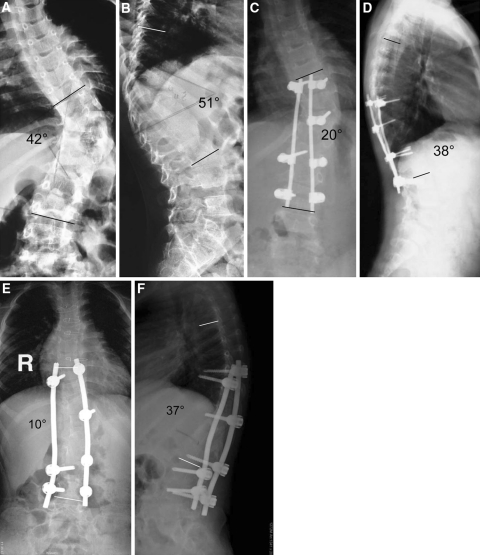
Thoracic pedicle screws have superior anchoring strength compared with other available fixation techniques. However, these are not universally accepted in many developing countries because of the concerns regarding safety and complications. In addition, there is evidence that pedicle morphology is unique in Chinese patients. The goal of this study was to analyze the complications seen at our institution, while using thoracic pedicle screws for the treatment of thoracic deformity, and to determine the safety of our techniques for the treatment of thoracic deformity in a Chinese population. From 1998 to 2005, there were 208 thoracic deformity patients treated at our institution, 70 of whom were male and 138 were female. Their age ranged from 11 to 55 years (mean of 14.9 years). All of them underwent corrective deformity surgery using posterior pedicle screw systems and follow-up was available for at least 3 years. Etiologic diagnoses included adolescent idiopathic scoliosis in 119 patients, congenital kyphoscoliosis in 38, adult scoliosis in 37 and undetermined in 14. Screw positions were evaluated using intraoperative and postoperative radiographs and a CT scan was performed when a concern for screw malposition was present. All radiographic evaluations were carried out in a double-blinded fashion. A total of 1,123 thoracic pedicle screws were inserted (5.4 thoracic screws/patient). The deformity correction rate was 81, 65 and 62% for idiopathic, congenital and adult scoliosis patients, respectively. The overall complication rate was 16.5% at the final follow-up. Complication rates directly and indirectly related to pedicle screws were 7.2 and 9.3%, respectively. There were no significant screw-related neurologic or visceral complications that adversely affected long-term results. The complications seen with thoracic pedicle screws in a Chinese population were similar to other populations and could be utilized safely for the treatment of thoracic deformity in this population.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
