

Low grade glandular lesions of the sinonasal tract: a focused review
- PMID: 20237993
- PMCID: PMC2825529
- DOI: 10.1007/s12105-009-0159-5
Low grade glandular lesions of the sinonasal tract: a focused review
Abstract
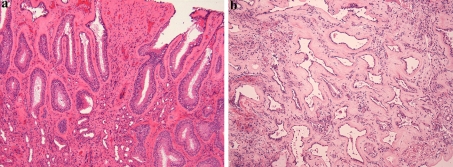
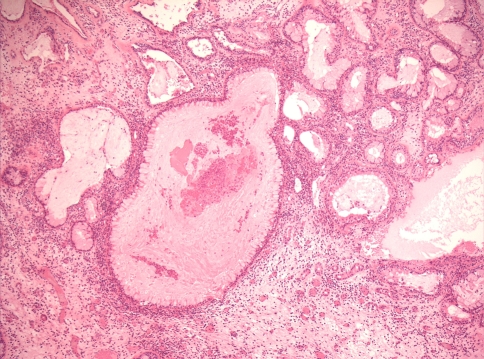
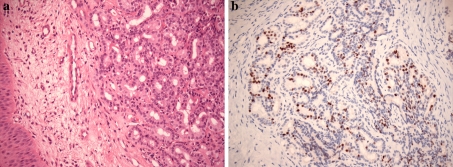
The sinonasal tract is a complex anatomic site with an exhaustive list of possible diagnoses. While most biopsies or resections encountered routinely consist of common diagnoses such as inflammatory polyps and papillomas, occasional cases are more difficult, and separating reactive or benign from malignancy can be challenging. One of the most poorly understood and daunting categories is low grade glandular or tubular proliferations, particularly on small biopsies. Possible diagnoses such as reactive lesions, respiratory epithelial adenomatoid hamartoma (REAH), seromucinous (glandular) hamartoma (SH) and low grade sinonasal adenocarcinomas (LGSNAC) must be entertained. REAH is composed of respiratory epithelial lined submucosal glands with variable connection to the surface and periglandular hyalinization. SH is a tubular proliferation reminiscent of normal serous glands which may be associated with REAH. LGSNAC is a diverse group of bland tubular and/or papillary tumors, which have a recurrence potential but an as yet uncertain potential for metastasis or mortality. The management for these lesions can be vastly different and conservative management is preferable, making this distinction more than academic. However, complicating this category are controversies surrounding their nature as reactive lesions versus neoplasms, the histologic and immunohistochemical overlap, and possible precursor relationships between some of them.
Figures



Similar articles
-
Immunohistochemical and genetic analysis of respiratory epithelial adenomatoid hamartomas and seromucinous hamartomas: are they precursor lesions to sinonasal low-grade tubulopapillary adenocarcinomas?Hum Pathol. 2020 Mar;97:94-102. doi: 10.1016/j.humpath.2019.09.018. Epub 2019 Nov 5. Hum Pathol. 2020. PMID: 31698004
-
Sinonasal Hamartomas.Surg Pathol Clin. 2024 Dec;17(4):577-585. doi: 10.1016/j.path.2024.07.001. Epub 2024 Aug 17. Surg Pathol Clin. 2024. PMID: 39489550 Review.
-
Low-Grade Epithelial Proliferations of the Sinonasal Tract.Head Neck Pathol. 2016 Mar;10(1):47-59. doi: 10.1007/s12105-016-0691-z. Epub 2016 Feb 1. Head Neck Pathol. 2016. PMID: 26830403 Free PMC article. Review.
-
Respiratory epithelial adenomatoid hamartoma associated with inflammatory nasal polyposis: a case report.Kulak Burun Bogaz Ihtis Derg. 2012 Jul-Aug;22(4):232-5. doi: 10.5606/kbbihtisas.2012.045. Kulak Burun Bogaz Ihtis Derg. 2012. PMID: 22770260
-
Sinonasal Hamartomas: From Nasal Chondromesenchymal Hamartoma to Respiratory Epithelial Adenomatoid Hamartoma. Report of six Cases and Review of the Literature.Int J Surg Pathol. 2022 Jun;30(4):448-456. doi: 10.1177/10668969211064211. Epub 2022 Jan 10. Int J Surg Pathol. 2022. PMID: 35001691 Review.
Cited by
-
Sinonasal seromucinous hamartoma: a review of the literature and a case report with focal myoepithelial cells.Head Neck Pathol. 2012 Sep;6(3):395-9. doi: 10.1007/s12105-012-0339-6. Epub 2012 Mar 6. Head Neck Pathol. 2012. PMID: 22392408 Free PMC article. Review.
-
Seromucinous hamartoma of inferior turbinate: A case report.Medicine (Baltimore). 2018 Nov;97(45):e13022. doi: 10.1097/MD.0000000000013022. Medicine (Baltimore). 2018. PMID: 30407294 Free PMC article.
-
Recently described sinonasal tract lesions/neoplasms: considerations for the new world health organization book.Head Neck Pathol. 2014 Mar;8(1):33-41. doi: 10.1007/s12105-014-0533-9. Epub 2014 Mar 5. Head Neck Pathol. 2014. PMID: 24595422 Free PMC article.
-
Seromucinous Hamartoma of the Lateral Nasal Wall with Infiltration of the Orbit: A Rare Case Report and Review of the Literature.Case Rep Otolaryngol. 2023 Aug 12;2023:1923015. doi: 10.1155/2023/1923015. eCollection 2023. Case Rep Otolaryngol. 2023. PMID: 37601823 Free PMC article.
-
Sinonasal Adenocarcinoma: Update on Classification, Immunophenotype and Molecular Features.Head Neck Pathol. 2016 Mar;10(1):68-74. doi: 10.1007/s12105-016-0694-9. Epub 2016 Feb 1. Head Neck Pathol. 2016. PMID: 26830399 Free PMC article. Review.
References
-
- Wenig BM, Heffner DK. Respiratory epithelial adenomatoid hamartomas of the sinonasal tract and nasopharynx: a clinicopathologic study of 31 cases. Ann Otol Rhinol Laryngol. 1995;104(8):639–645. - PubMed
-
- Wenig BM. Respiratory epithelial adenomatoid hamartoma. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors. World Health Organization Classification of Tumours. Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
