

The many faces of multivisceral transplantation
- PMID: 2028370
- PMCID: PMC2655210
The many faces of multivisceral transplantation
Erratum in
- Surg Gynecol Obstet 1991 Sep;173(3):242
Abstract
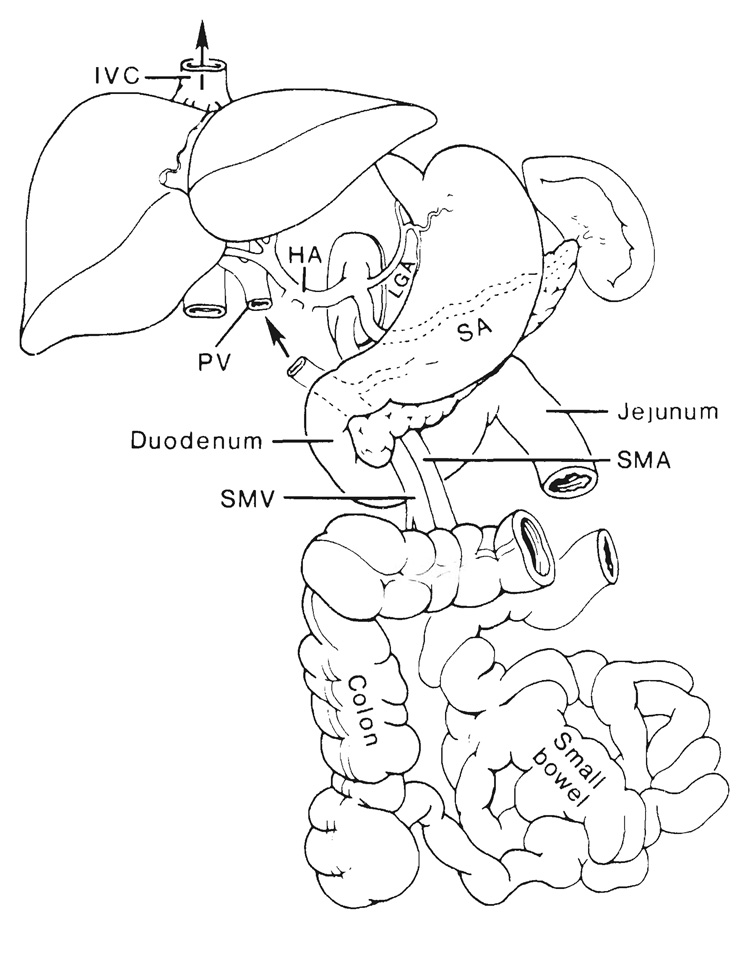
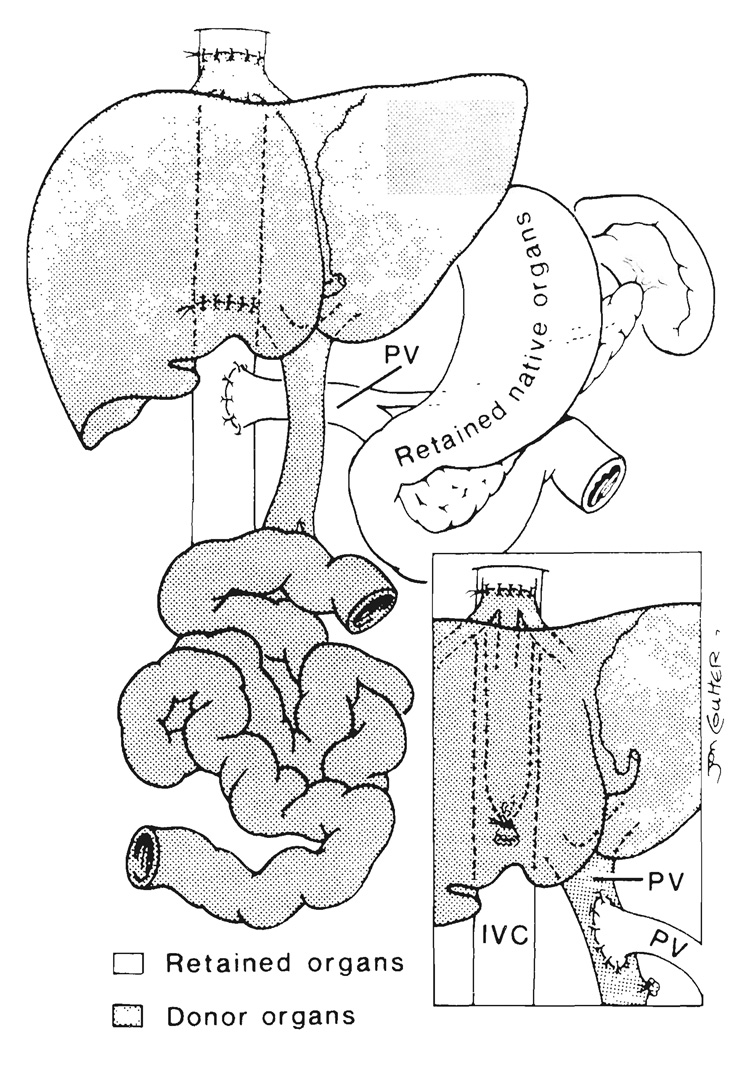
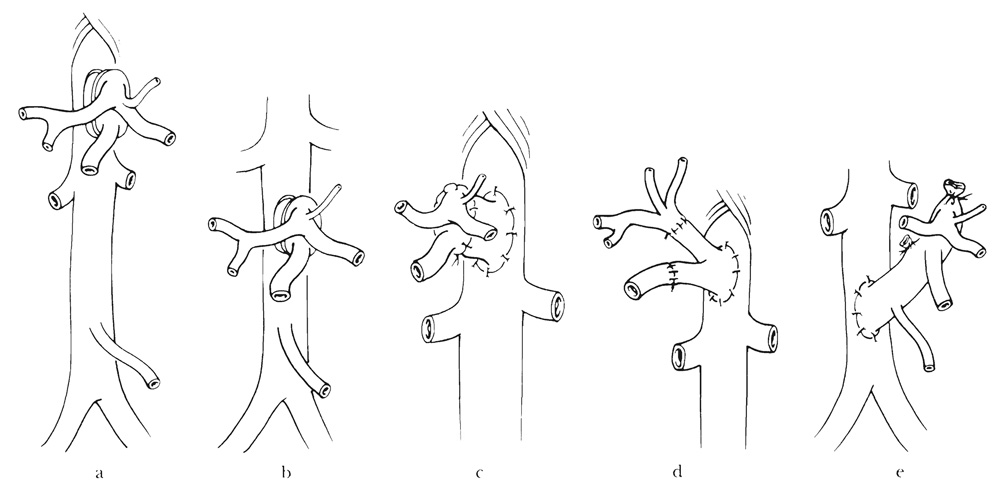
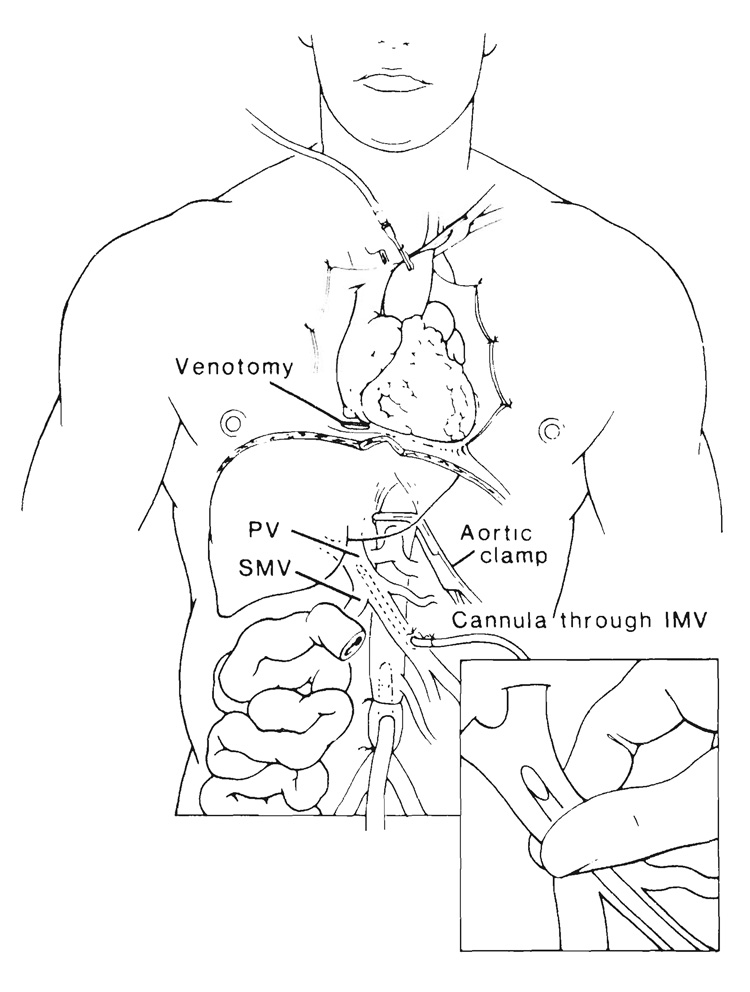
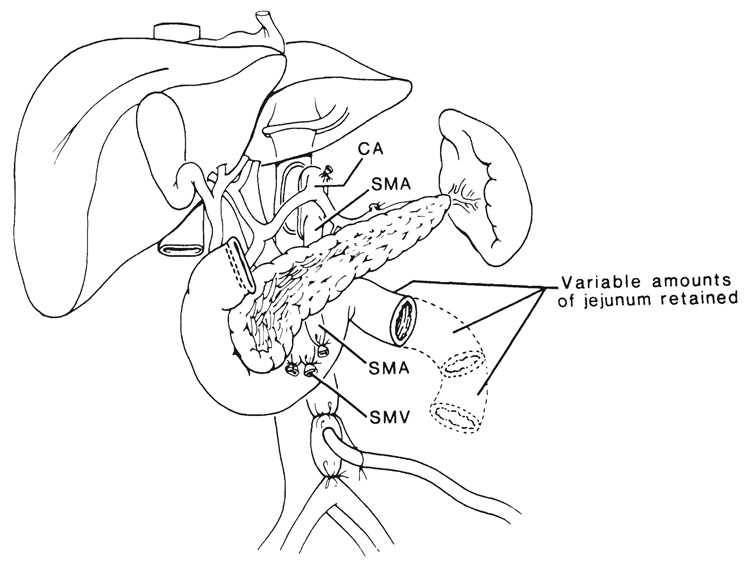
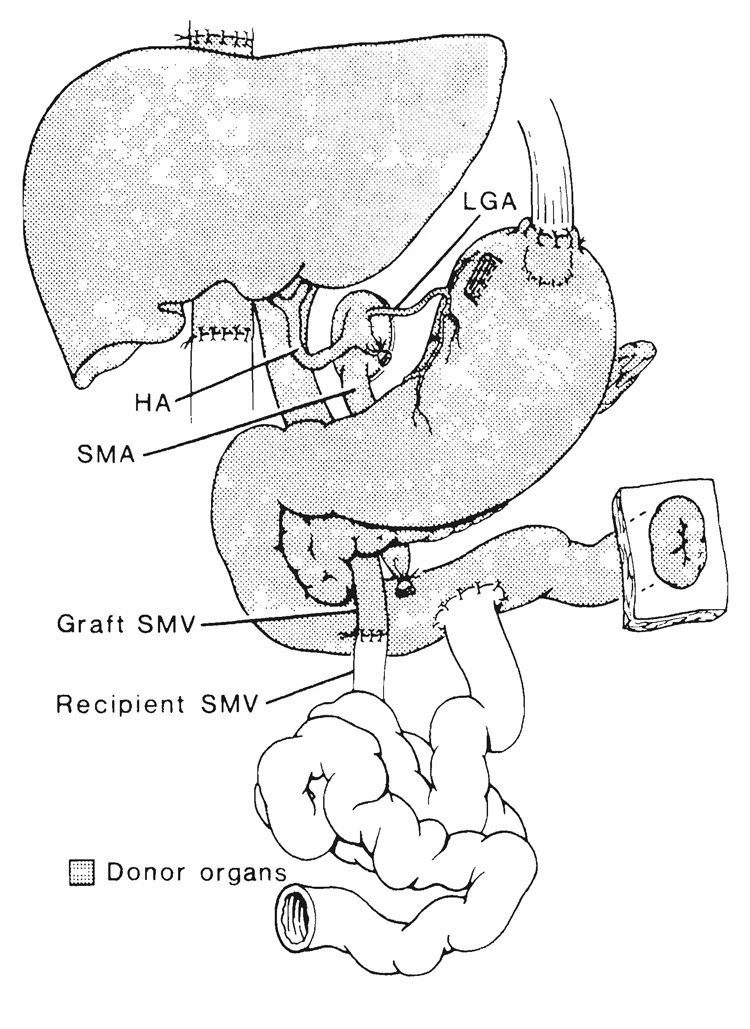
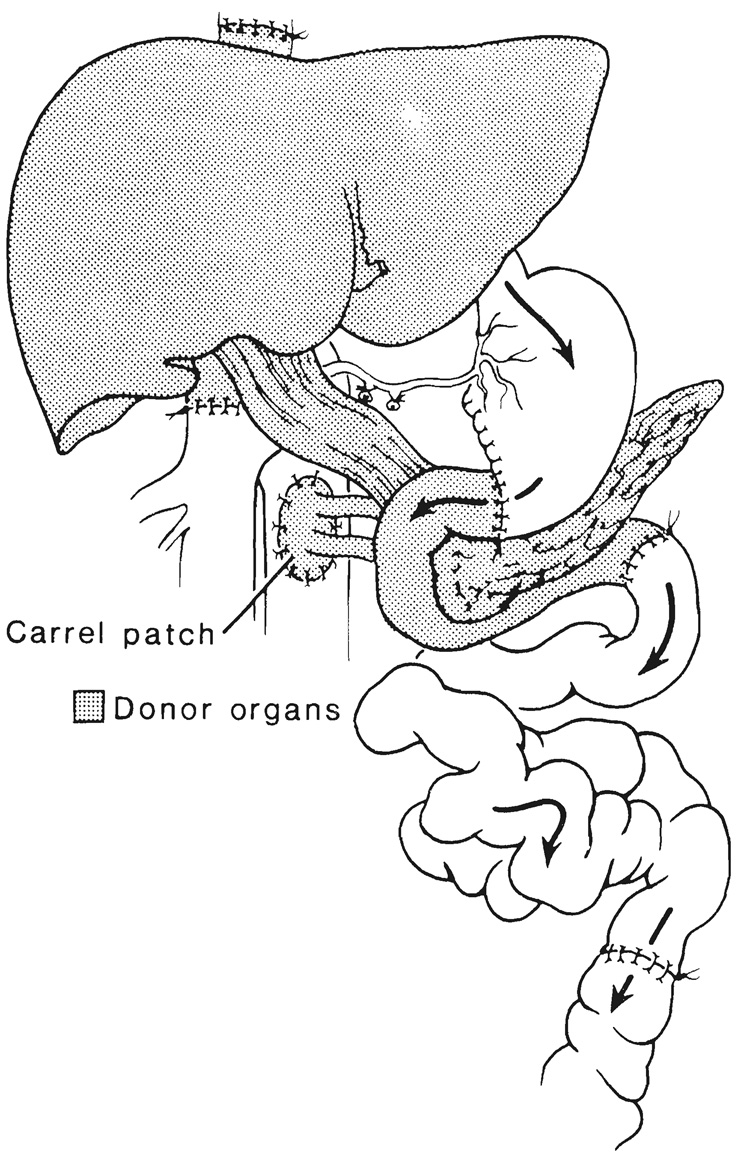
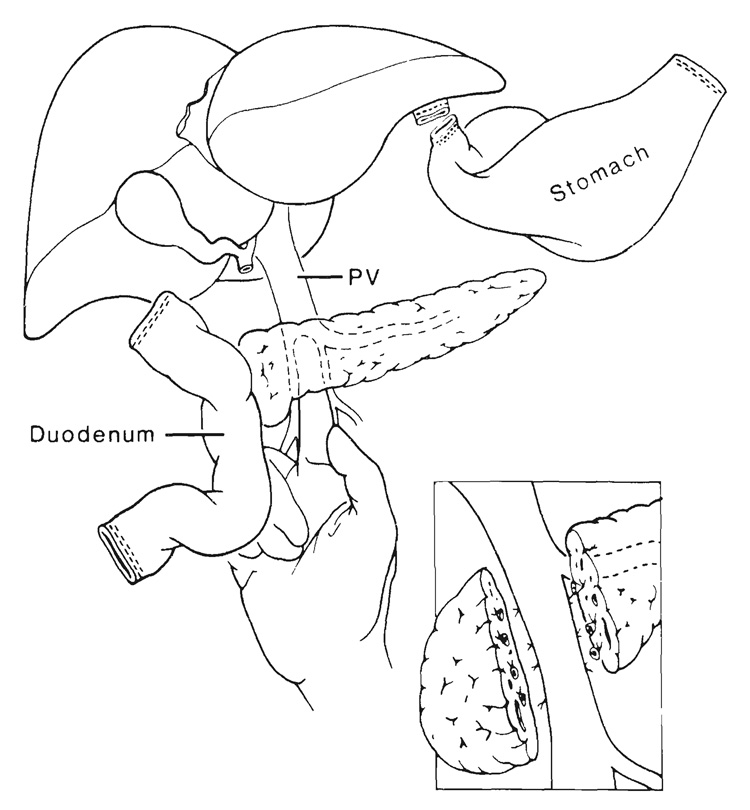
The transplantation of multiple abdominal viscera, including liver-duodenum-pancreas, liver-stomach-duodenum-pancreas and liver-intestine, is being performed with increasing frequency and success. These procedures and other variations are derived from a seldom used multivisceral operation in which all of the foregoing organs are transplanted en bloc. It is described herein how the full multivisceral transplantation and its less extensive derivatives are based on the same principles of procurement, preservation and postoperative management. With all of these multiple organ permutations and with intestinal transplantation alone, management is complicated by inclusion in the grafts of a large lymphoreticular component that is capable of causing graft versus host disease (GVHD). Because of a systematic error in therapeutic philosophy, past efforts have been directed at altering or damaging the lymphoreticular cells by pretreatment of the donor or of the organs with drugs, irradiation or other means. From recent observations, the alternative approach is suggested of keeping these lymphoid depots intact, which then become the site of two way cell traffic after transplantation. With the use of powerful immunosuppression, such as that provided with FK 506, the donor lymphoreticular cells can circulate in the recipient without causing clinical GVHD, and the lymphoreticular cells in the graft become those of the recipient (local chimerism) without causing rejection. Even with avoidance of rejection and GVHD, metabolic interrelations between the grafted organs, and also between the graft organs and retained recipient viscera can affect the fate of the individual transplanted organs or retained recipient organs. The best delineated of these metabolic influences are mediated by the endogenous splanchnic hepatotrophic factors, of which insulin has been the most completely studied. An understanding of these various immunologic and nonimmunologic factors combined with more potent immunosuppression that is now available is sure to stimulate efforts at transplantation of abdominal organs and particularly of the hollow viscera that have resisted such clinical efforts.
Figures

References
-
- Jaffe BM. Visceral interchange. Am. J. Surg. 1989;157:2–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous