

Effect of smoking on lung function, respiratory symptoms and respiratory diseases amongst HIV-positive subjects: a cross-sectional study
- PMID: 20298614
- PMCID: PMC2853483
- DOI: 10.1186/1742-6405-7-6
Effect of smoking on lung function, respiratory symptoms and respiratory diseases amongst HIV-positive subjects: a cross-sectional study
Abstract
Background: Smoking prevalence in human immunodeficiency virus (HIV) positive subjects is about three times of that in the general population. However, whether the extremely high smoking prevalence in HIV-positive subjects affects their lung function is unclear, particularly whether smoking decreases lung function more in HIV-positive subjects, compared to the general population. We conducted this study to determine the association between smoking and lung function, respiratory symptoms and diseases amongst HIV-positive subjects.
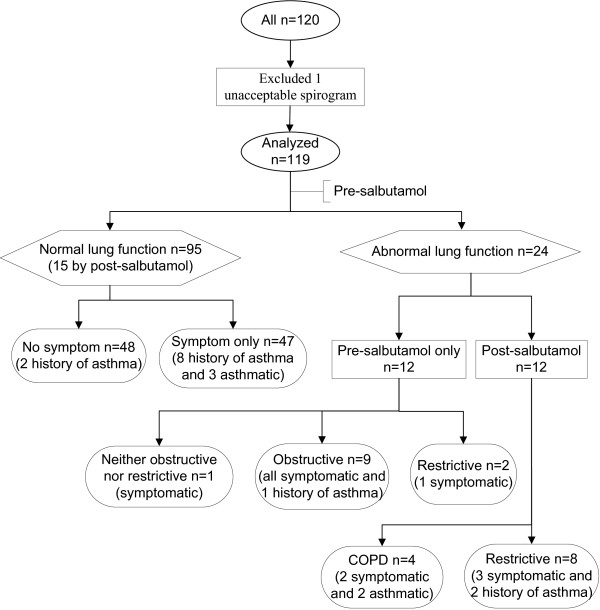
Results: Of 120 enrolled HIV-positive subjects, 119 had an acceptable spirogram. Ninety-four (79%) subjects were men, and 96 (81%) were white. Mean (standard deviation [SD]) age was 43.4 (8.4) years. Mean (SD) of forced expiratory volume in one second (FEV1) percent of age, gender, race and height predicted value (%FEV1) was 93.1% (15.7%). Seventy-five (63%) subjects had smoked 24.0 (18.0) pack-years. For every ten pack-years of smoking increment, %FEV1 decreased by 2.1% (95% confidence interval [CI]: -3.6%, -0.6%), after controlling for gender, race and restrictive lung function (R2 = 0.210). The loss of %FEV1 in our subjects was comparable to the general population. Compared to non-smokers, current smokers had higher odds of cough, sputum or breathlessness, after adjusting for highly active anti-retroviral therapy (HAART) use, odds ratio OR = 4.9 (95% CI: 2.0, 11.8). However respiratory symptom presence was similar between non-smokers and former smokers, OR = 1.0 (95% CI: 0.3, 2.8). All four cases of COPD (chronic obstructive pulmonary disease) had smoked. Four of ten cases of restrictive lung disease had smoked (p = 0.170), and three of five asthmatic subjects had smoked (p = 1.000).
Conclusions: Cumulative cigarette consumption was associated with worse lung function; however the loss of %FEV1 did not accelerate in HIV-positive population compared to the general population. Current smokers had higher odds of respiratory symptoms than non-smokers, while former smokers had the same odds of respiratory symptoms as non-smokers. Cigarette consumption was likely associated with more COPD cases in HIV-positive population; however more participants and longer follow up would be needed to estimate the effect of smoking on COPD development. Effective smoking cessation strategies are required for HIV-positive subjects.
Figures
References
-
- Canadian Tobacco Use Monitoring Survey (CTUMS) Archives 1999 - 2007. http://www.hc-sc.gc.ca/hc-ps/tobac-tabac/research-recherche/stat/index-e...
-
- Poirier CD, Inhaber N, Lalonde RG, Ernst P. Prevalence of bronchial hyperresponsiveness among HIV-infected men. Am J Respir Crit Care Med. 2001;164:542–545. - PubMed
-
- Miguez-Burbano MJ, Ashkin D, Rodriguez A, Duncan R, Pitchenik A, Quintero N, Flores M, Shor-Posner G. Increased risk of pneumocystis carinii and community-acquired pneumonia with tobacco use in HIV disease. International Journal of Infectious Diseases. 2005;9:208–217. doi: 10.1016/j.ijid.2004.07.010. - DOI - PubMed
-
- Diaz P, King M, Pacht E, Wewers M, Gadek J, Nagaraja H, Drake J, Clanton T. Increased susceptibility to pulmonary emphysema among HIV-seropositive smokers. Annals of Internal Medicine. 2000;132:369–372. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
