

Utility of functional status for classifying community versus institutional discharges after inpatient rehabilitation for stroke
- PMID: 20298822
- PMCID: PMC2896793
- DOI: 10.1016/j.apmr.2009.11.010
Utility of functional status for classifying community versus institutional discharges after inpatient rehabilitation for stroke
Abstract
Objective: To evaluate the ability of patient functional status to differentiate between community and institutional discharges after rehabilitation for stroke.
Design: Retrospective cross-sectional design.
Setting: Inpatient rehabilitation facilities contributing to the Uniform Data System for Medical Rehabilitation.
Participants: Patients (N=157,066) receiving inpatient rehabilitation for stroke from 2006 and 2007.
Interventions: Not applicable.
Main outcome measure: Discharge FIM rating and discharge setting (community vs institutional).
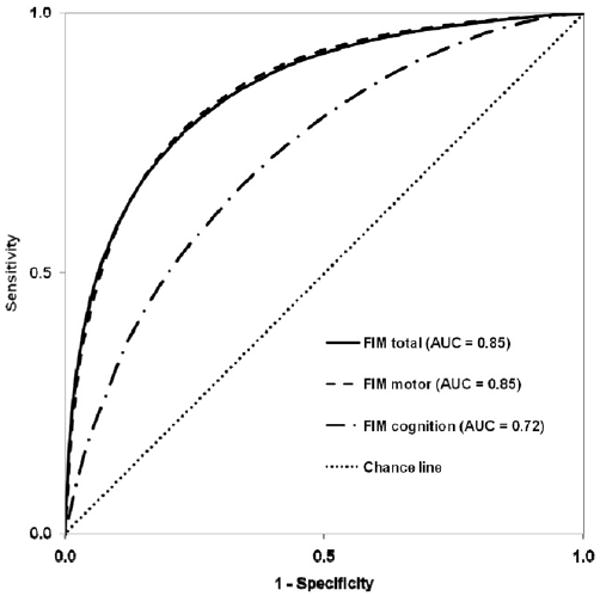
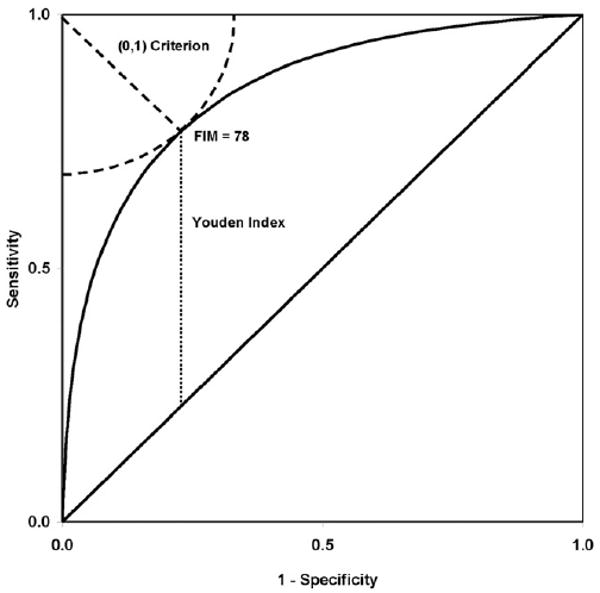
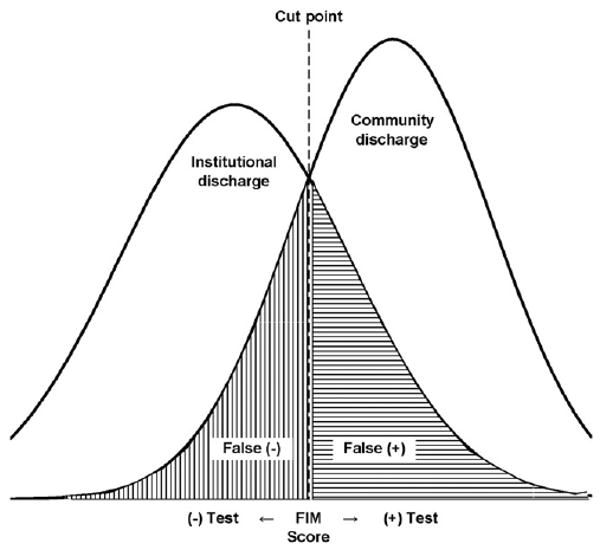
Results: Approximately 71% of the sample was discharged to the community. Receiver operating characteristic curve analyses revealed that FIM total performed as well as or better than FIM motor and FIM cognition subscales in differentiating discharge settings. Area under the curve for FIM total was .85, indicating very good ability to identify persons discharged to the community. A FIM total rating of 78 was identified as the optimal cut point for distinguishing between positive (community) and negative (institution) tests. This cut point yielded balanced sensitivity and specificity (both=.77).
Conclusions: Discharge planning is complex, involving many factors. Identifying a functional threshold for classifying discharge settings can provide important information to assist in this process. Additional research is needed to determine if the risks and benefits of classification errors justify shifting the cut point to weight either sensitivity or specificity of FIM ratings.
Copyright 2010 American Congress of Rehabilitation Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
A commercial party having a direct financial interest in the results of the research supporting this article has conferred or will confer a financial benefit on the author or one or more of the authors. Granger is an employee of the State University of New York at Buffalo and serves as the Executive Director of the Uniform Data System for Medical Rehabilitation, a division of the UB Foundation Activities, Inc. Markello is an employee of the UB Foundation Activities, Inc. and serves as the Associate Director of the Uniform Data System for Medical Rehabilitation, a division of the UB Foundation Activities, Inc. UB Foundation Activities, Inc. owns the copyright and trademark for the FIM Instrument.
Figures
Similar articles
-
FIM motor scores for classifying community discharge after inpatient rehabilitation for hip fracture.PM R. 2014 Jun;6(6):493-7. doi: 10.1016/j.pmrj.2013.12.008. Epub 2013 Dec 31. PM R. 2014. PMID: 24389348 Free PMC article.
-
The uniform data system for medical rehabilitation: report of patients with traumatic spinal cord injury discharged from rehabilitation programs in 2002-2010.Am J Phys Med Rehabil. 2012 Apr;91(4):289-99. doi: 10.1097/PHM.0b013e31824ad2fd. Am J Phys Med Rehabil. 2012. PMID: 22407160 Free PMC article.
-
Functional Independence predicts patients with stroke more likely to be discharged to the community after inpatient rehabilitation.Top Stroke Rehabil. 2023 May;30(4):393-401. doi: 10.1080/10749357.2022.2038834. Epub 2022 Feb 14. Top Stroke Rehabil. 2023. PMID: 35156558
-
Predicting goal achievement during stroke rehabilitation for Medicare beneficiaries.Disabil Rehabil. 2014;36(15):1273-8. doi: 10.3109/09638288.2013.845253. Epub 2013 Oct 23. Disabil Rehabil. 2014. PMID: 24151817
-
A retrospective observational study of functional outcomes, length of stay, and discharge disposition after an inpatient stroke rehabilitation program in Saudi Arabia.Medicine (Baltimore). 2016 Aug;95(31):e4432. doi: 10.1097/MD.0000000000004432. Medicine (Baltimore). 2016. PMID: 27495066 Free PMC article.
Cited by
-
Successful Community Discharge Among Older Adults With Traumatic Brain Injury Admitted to Inpatient Rehabilitation Facilities.Arch Rehabil Res Clin Transl. 2022 Nov 1;4(4):100241. doi: 10.1016/j.arrct.2022.100241. eCollection 2022 Dec. Arch Rehabil Res Clin Transl. 2022. PMID: 36545522 Free PMC article.
-
A retrospective study on return to living alone of stroke patients who were living alone before stroke.J Phys Ther Sci. 2023 Jun;35(6):440-446. doi: 10.1589/jpts.35.440. Epub 2023 Jun 1. J Phys Ther Sci. 2023. PMID: 37266369 Free PMC article.
-
Regional variation in stroke rehabilitation outcomes.Arch Phys Med Rehabil. 2014 Jan;95(1):29-38. doi: 10.1016/j.apmr.2013.07.018. Epub 2013 Aug 3. Arch Phys Med Rehabil. 2014. PMID: 23921200 Free PMC article.
-
Development and Validation of a Decision Tree Analysis Model for Predicting Home Discharge in a Convalescent Ward: A Single Institution Study.Phys Ther Res. 2024;27(1):14-20. doi: 10.1298/ptr.E10267. Epub 2024 Jan 19. Phys Ther Res. 2024. PMID: 38690531 Free PMC article.
-
Clarification of Factors Determining Discharge Destination Among Elderly Patients After Stroke With Low Levels of Independence in Activities of Daily Living: A Retrospective Study.Arch Rehabil Res Clin Transl. 2022 Aug 7;4(4):100226. doi: 10.1016/j.arrct.2022.100226. eCollection 2022 Dec. Arch Rehabil Res Clin Transl. 2022. PMID: 36545528 Free PMC article.
References
-
- UB Foundation Activities. Centers for Medicare and Medicaid Services; [December 3, 2009]. The IRF-PAI Training Manual. Available at: http://www.cms.hhs.gov/InpatientRehabFacPPS/downloads/irfpaimanual040104....
-
- DeJong G, Branch LG. Predicting the stroke patient's ability to live independently. Stroke. 1982;13:648–55. - PubMed
-
- Lutz BJ. Determinants of discharge destination for stroke patients. Rehabil Nurs. 2004;29:154–63. - PubMed
-
- Nguyen TA, Page A, Aggarwal A, Henke P. Social determinants of discharge destination for patients after stroke with low admission FIM instrument scores. Arch Phys Med Rehabil. 2007;88:740–4. - PubMed
-
- Unsworth CA, Thomas SA, Greenwood KM. Rehabilitation teams decisions on discharge housing for stroke patients. Arch Phys Med Rehabil. 1995;76:331–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
