

The indeterminate adrenal lesion
- PMID: 20299300
- PMCID: PMC2842175
- DOI: 10.1102/1470-7330.2010.0012
The indeterminate adrenal lesion
Abstract
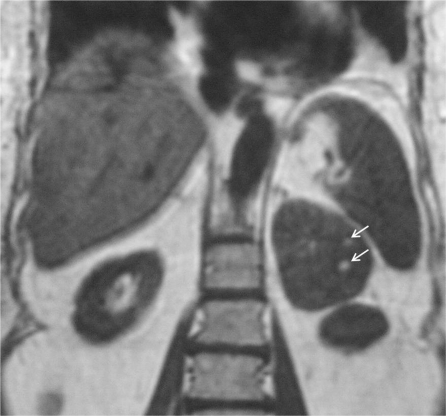
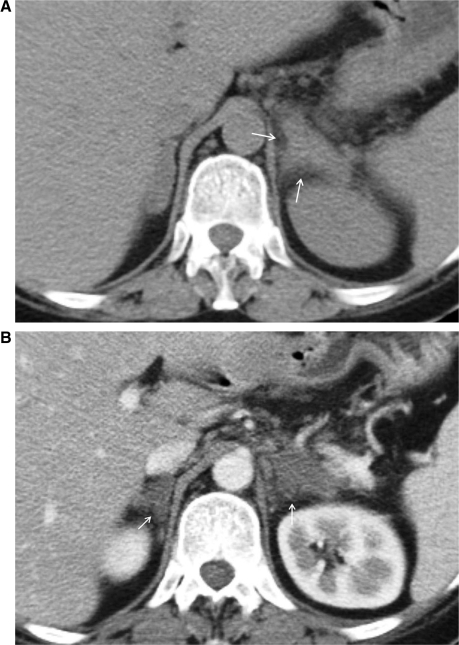
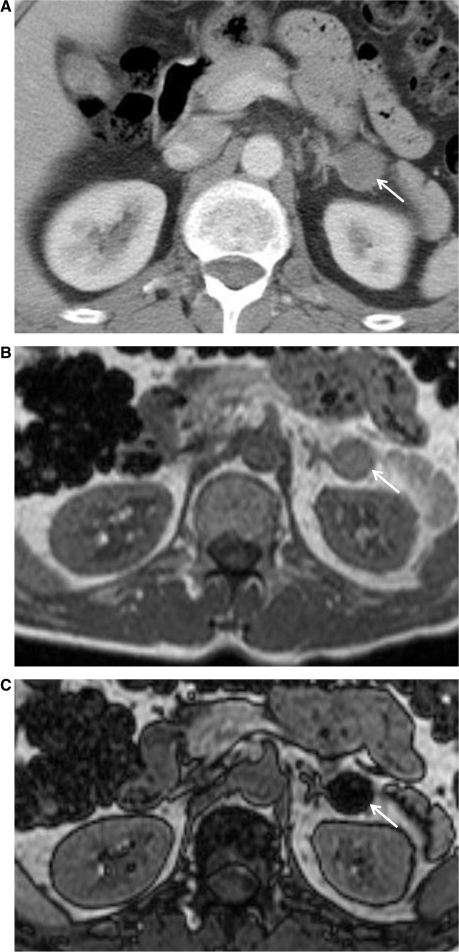
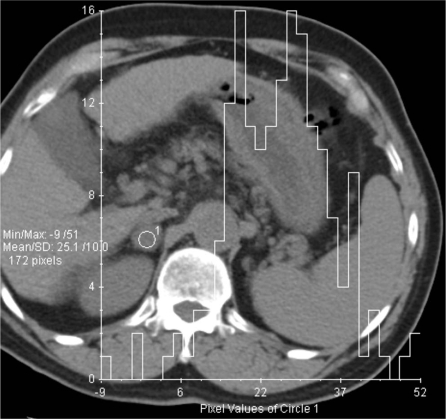
With the increasing use of abdominal cross-sectional imaging, incidental adrenal masses are being detected more often. The important clinical question is whether these lesions are benign adenomas or malignant primary or secondary masses. Benign adrenal masses such as lipid-rich adenomas, myelolipomas, adrenal cysts and adrenal haemorrhage have pathognomonic cross-sectional imaging appearances. However, there remains a significant overlap between imaging features of some lipid-poor adenomas and malignant lesions. The nature of incidentally detected adrenal masses can be determined with a high degree of accuracy using computed tomography (CT) and magnetic resonance imaging (MRI) alone. Positron emission tomography (PET) is also increasingly used in clinical practice in characterizing incidentally detected lesions. We review the performance of the established and new techniques in CT, MRI and PET that can be used to distinguish benign adenomas and malignant lesions of the adrenal gland.
Figures




References
-
- Glazer HS, Weyman PJ, Sagel SS, Levitt RG, McClennan BL. Non-functioning adrenal masses: incidental discovery on computed tomography. AJR. 1982;139:81–5. - PubMed
-
- Bovio S, Cataldi A, Reimondo G, et al. Prevalence of adrenal incidentaloma in a contemporary computerized tomography series. J Endocrinol Invest. 2006;29:298–302. - PubMed
-
- Song JH, Chaudhry FS, Mayo-Smith WW. The incidental adrenal mass on CT: prevalence of adrenal disease in 1,049 consecutive adrenal masses in patients with no known malignancy. AJR. 2008;190:1163–8. doi:10.2214/AJR.07.2799. PMid:18430826. - DOI - PubMed
-
- Libe R, Bertherat J. Molecular genetics of adrenocortical tumours, from familial to sporadic diseases. Eur J Endocrinol. 2005;153:477–87. doi:10.1530/eje.1.02004. PMid:16189167. - DOI - PubMed
-
- Oliver TW, Jr, Bernardino ME, Miller JI, Mansour K, Greene D, Davis WA. Isolated adrenal masses in non small-cell bronchogenic carcinoma. Radiology. 1984;153:217–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical