

Case Reports
doi: 10.1102/1470-7330.2010.0015.
FDG-PET/CT findings of a metastatic pituitary tumor
Affiliations
- PMID: 20299302
- PMCID: PMC2842182
- DOI: 10.1102/1470-7330.2010.0015
Item in Clipboard
Case Reports
FDG-PET/CT findings of a metastatic pituitary tumor
Cancer Imaging.
.
Abstract
The authors report the fluorodeoxyglucose (FDG)-positron emission tomography(PET)/computed tomography (CT) findings of a rare case of growth hormone-secreting pituitary carcinoma with multiple metastatic lesions to the skeleton. A 31-year-old male had presented with acromegaly and had received transsphenoidal resection of a pituitary tumor and adjuvant radiotherapy. However, the tumor recurred with local invasions and the patient underwent more resections and adjuvant chemotherapy. Several months later, the patient developed rising levels of insulin-like growth factor 1 and whole-body FDG-PET/CT scanning revealed multiple hypermetabolic lesions throughout the skeleton compatible with metastasis.
Figures

(A) T1-weighted MR imaging (spin echo, repetition time (TR)/echo time (TE)=466.7 ms/13 ms) with contrast enhancement of the head shows an enhancing mass in the sella turcica extending to the right cavernous sinus, consistent with local recurrence of tumor. (B) Whole-body FDG-PET/CT fusion image in the same level shows abnormal increased FDG uptake of tumor (large arrow) and physiological uptake of right temporal lobe (small arrow).
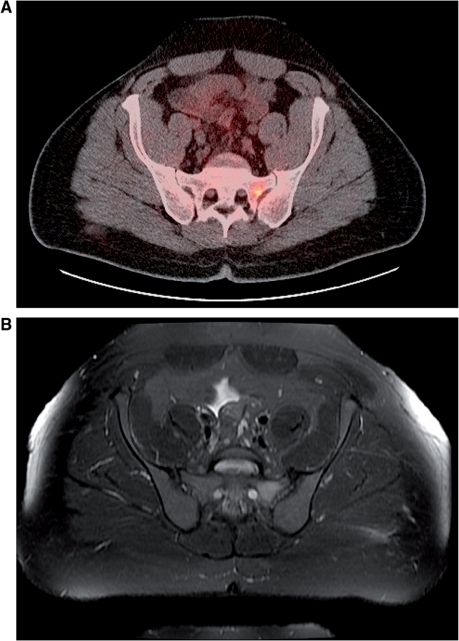
(A) Whole-body FDG-PET/CT fusion image shows an area of increased FDG uptake in the left sacral ala, consistent with metastatic tumor. (B) The T2-weighted MR imaging (fast-spin echo, TR/TE/echo train length=5200 ms/72 ms/17) with fat saturation shows increased T2 signal intensity in the same area.
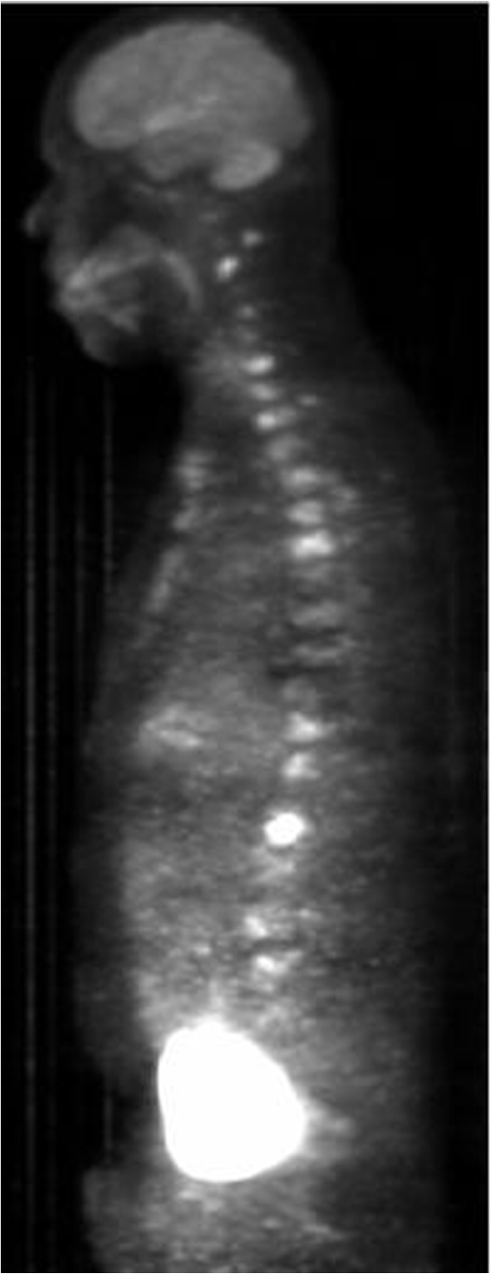
PET/CT maximum intensity projection image showing numerous foci of increased tracer uptake in the cervical, thoracic, lumbar spine, and sternum, consistent with metastatic disease.
Similar articles
-
[F-18]fluorodeoxyglucose positron emission tomography and positron emission tomography: computed tomography in recurrent and metastatic cholangiocarcinoma.J Comput Assist Tomogr. 2007 Mar-Apr;31(2):223-8. doi: 10.1097/01.rct.0000237811.88251.d7. J Comput Assist Tomogr. 2007. PMID: 17414758
-
Positron emission tomography and bone metastases.Semin Nucl Med. 2005 Apr;35(2):135-42. doi: 10.1053/j.semnuclmed.2004.11.005. Semin Nucl Med. 2005. PMID: 15765376 Review.
-
Fusion of metabolic function and morphology: sequential [18F]fluorodeoxyglucose positron-emission tomography/computed tomography studies yield new insights into the natural history of bone metastases in breast cancer.J Clin Oncol. 2007 Aug 10;25(23):3440-7. doi: 10.1200/JCO.2007.11.2854. Epub 2007 Jun 25. J Clin Oncol. 2007. PMID: 17592153
-
FDG-anorectic parathyroid carcinoma with FDG-avid bone metastasis on PET/CT images.Clin Nucl Med. 2013 Nov;38(11):916-8. doi: 10.1097/RLU.0b013e3182a757fd. Clin Nucl Med. 2013. PMID: 24089062
-
PET/CT in benign and malignant musculoskeletal tumors and tumor-like conditions.Semin Musculoskelet Radiol. 2014 Apr;18(2):133-48. doi: 10.1055/s-0034-1371016. Epub 2014 Apr 8. Semin Musculoskelet Radiol. 2014. PMID: 24715446 Review.
Cited by
-
A Pituitary Carcinoma Patient With Cerebrospinal Fluid Dissemination Showing a Good Response to Temozolomide Combined With Whole-Brain and Spinal Cord Radiotherapy: A Case Report and Literature Review.Front Oncol. 2022 Jul 12;12:890458. doi: 10.3389/fonc.2022.890458. eCollection 2022. Front Oncol. 2022. PMID: 35903687 Free PMC article.
-
Corticotrophic pituitary carcinoma with cervical metastases: case series and literature review.Pituitary. 2018 Jun;21(3):290-301. doi: 10.1007/s11102-018-0872-8. Pituitary. 2018. PMID: 29404894 Review.
-
Orbital metastasis of pituitary growth hormone secreting carcinoma causing lateral gaze palsy.Surg Neurol Int. 2013 Apr 18;4:59. doi: 10.4103/2152-7806.110658. Print 2013. Surg Neurol Int. 2013. PMID: 23646269 Free PMC article.
-
Imaging and clinical course of metastatic pituitary neuroendocrine tumors (PitNET): A single center case series.Neuroradiol J. 2025 Jun 27:19714009251356278. doi: 10.1177/19714009251356278. Online ahead of print. Neuroradiol J. 2025. PMID: 40576016 Free PMC article.
-
Clinical features of pituitary carcinoma: analysis based on a case report and literature review.Front Endocrinol (Lausanne). 2024 Oct 31;15:1440247. doi: 10.3389/fendo.2024.1440247. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39544231 Free PMC article. Review.
References
-
- Pernicone PJ, Scheithauer BW, Sebo TJ, et al. Pituitary carcinoma, a clinicopathologic study of 15 cases. Cancer. 1997;79:804–12. doi:10.1002/(SICI)1097-0142(19970215)79:4<804::AID-CNCR18>3.0.CO;2-3. - DOI - PubMed
-
- Cairns H, Russel DS. Intracranial and spinal metastasis in gliomas of the brain. Brain. 1931;54:377–420.
-
- Long MA, Colquhoun IR. Case report: multiple intracranial metastases from a prolactin-secreting pituitary tumor. Clin Radiol. 1994;49:356–8. doi:10.1016/S0009-9260(05)81807-0. - DOI - PubMed
-
- Ragel BT, Couldwell WT. Pituitary carcinoma: a review of literature. Neurosurg Focus. 2004;16 doi:10.3171/foc.2004.16.4.8. - DOI - PubMed
-
- Kaltas GA, Nomikos P, Kontogeorgos G, Buchfelder M. Clinical review: diagnosis and management of pituitary carcinomas. J Clin Endocrinol Metab. 2005;90:3089–99. doi:10.1210/jc.2004-2231. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical