

Outcome predictability of serum alkaline phosphatase in men with pre-dialysis CKD
- PMID: 20299338
- PMCID: PMC2948834
- DOI: 10.1093/ndt/gfq144
Outcome predictability of serum alkaline phosphatase in men with pre-dialysis CKD
Abstract
Background: Serum alkaline phosphatase (ALP) increases in patients with chronic kidney disease (CKD) and high-turnover bone disease. ALP may represent an adjunct marker of high bone turnover devoid of drawbacks of serum parathyroid hormone (PTH), and it may also be associated with cardiovascular calcification in CKD. Higher ALP has been recently associated with increased mortality and coronary calcification in dialysis patients. In pre-dialysis CKD patients, this association is not clear.
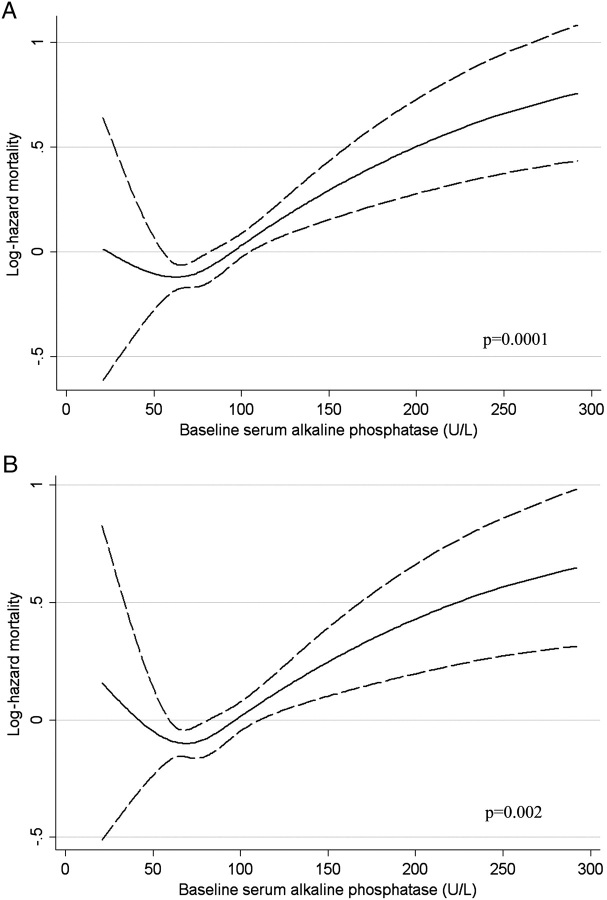
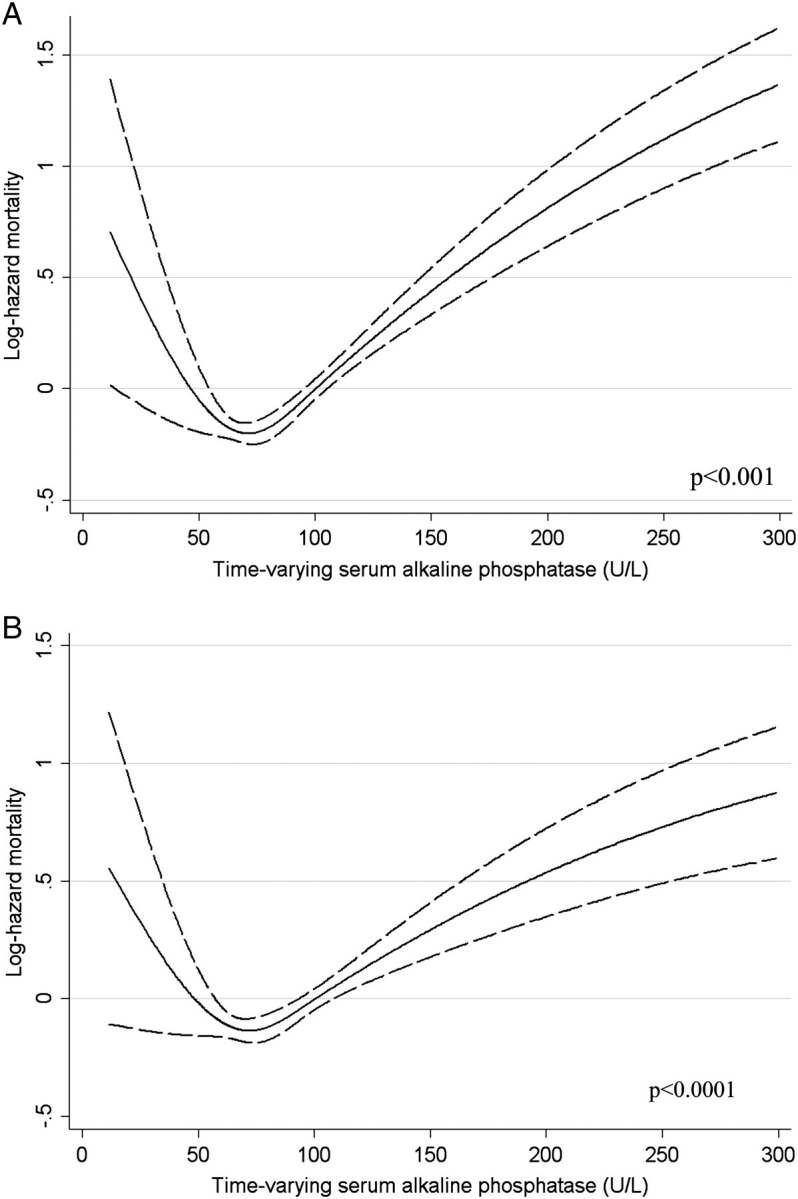
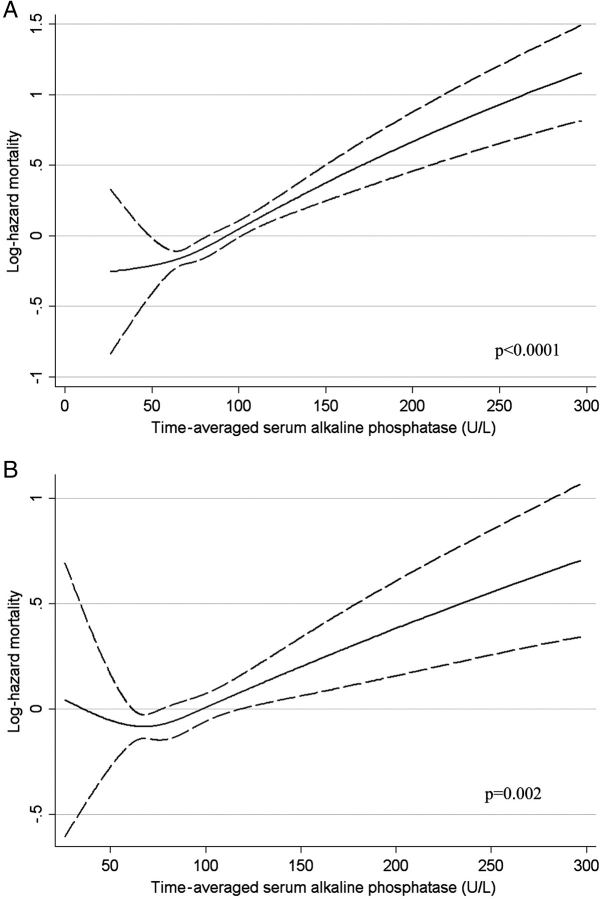
Methods: We examined the association of baseline, time-varying and time-averaged ALP with all-cause mortality and the composite of pre-dialysis mortality or end-stage renal disease in a historical prospective cohort of 1158 male veterans with pre-dialysis CKD from a single institution by using multivariable-adjusted Cox models.
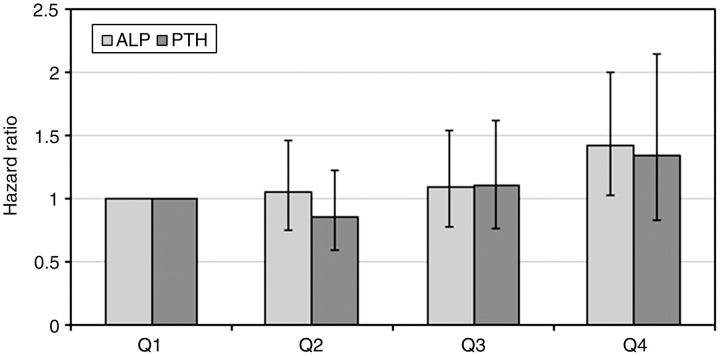
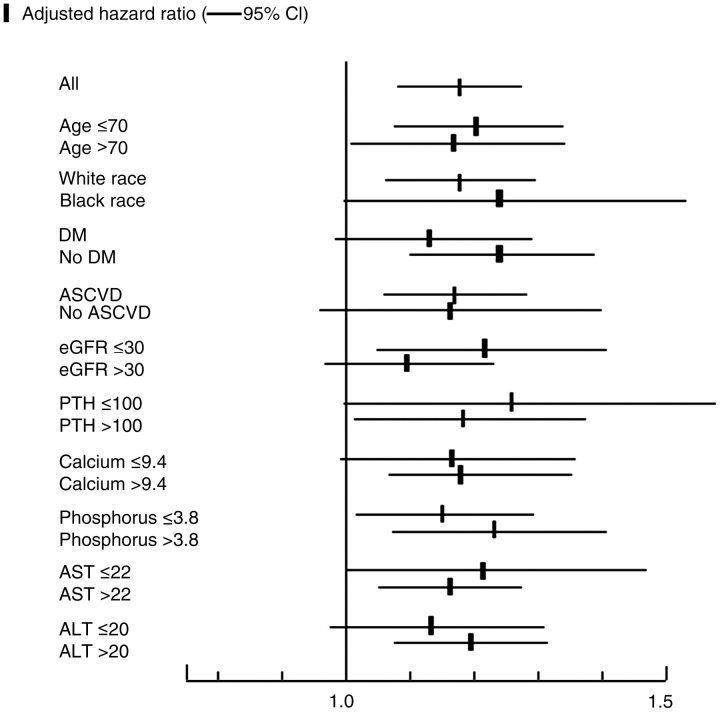
Results: Higher ALP was associated with increased mortality irrespective of the statistical model. Time-averaged ALP displayed a consistent linear association with mortality: a 50-U/L higher serum ALP was associated with a multivariable-adjusted death hazard ratio (95% confidence interval) of 1.17 (1.08-1.28), P < 0.001. Baseline and time-varying ALP showed non-linear associations with mortality, with serum levels above 70 U/L in all models and with lower levels in time-varying models. Associations between ALP levels and the composite outcomes were similar. However, compared to serum PTH, mortality predictability of ALP appeared more incremental.
Conclusions: Elevated ALP is associated with increased mortality in patients with pre-dialysis CKD. Low ALP appears to be associated with short-term mortality.
Figures
Similar articles
-
Prognostic significance of pre-end-stage renal disease serum alkaline phosphatase for post-end-stage renal disease mortality in late-stage chronic kidney disease patients transitioning to dialysis.Nephrol Dial Transplant. 2018 Feb 1;33(2):264-273. doi: 10.1093/ndt/gfw412. Nephrol Dial Transplant. 2018. PMID: 28064159 Free PMC article.
-
Comparative mortality-predictability using alkaline phosphatase and parathyroid hormone in patients on peritoneal dialysis and hemodialysis.Perit Dial Int. 2014 Nov-Dec;34(7):732-48. doi: 10.3747/pdi.2013.00110. Epub 2014 Jan 2. Perit Dial Int. 2014. PMID: 24385335 Free PMC article.
-
Effect Modifying Role of Serum Calcium on Mortality-Predictability of PTH and Alkaline Phosphatase in Hemodialysis Patients: An Investigation Using Data from the Taiwan Renal Registry Data System from 2005 to 2012.PLoS One. 2015 Jun 24;10(6):e0129737. doi: 10.1371/journal.pone.0129737. eCollection 2015. PLoS One. 2015. PMID: 26107510 Free PMC article.
-
Bone alkaline phosphatase in CKD-mineral bone disorder.Am J Kidney Dis. 2013 Oct;62(4):810-22. doi: 10.1053/j.ajkd.2013.02.366. Epub 2013 Apr 23. Am J Kidney Dis. 2013. PMID: 23623575 Review.
-
Alkaline phosphatase: a novel treatment target for cardiovascular disease in CKD.Nat Rev Nephrol. 2017 Jul;13(7):429-442. doi: 10.1038/nrneph.2017.60. Epub 2017 May 15. Nat Rev Nephrol. 2017. PMID: 28502983 Review.
Cited by
-
Genetic-Variation-Driven Gene-Expression Changes Highlight Genes with Important Functions for Kidney Disease.Am J Hum Genet. 2017 Jun 1;100(6):940-953. doi: 10.1016/j.ajhg.2017.05.004. Am J Hum Genet. 2017. PMID: 28575649 Free PMC article.
-
Relationship between serum alkaline phosphatase and poor 3-month prognosis in acute ischemic stroke patients with preserved renal function: results from Xi'an Stroke Registry Study of China.BMC Neurol. 2022 Jul 7;22(1):249. doi: 10.1186/s12883-022-02779-y. BMC Neurol. 2022. PMID: 35799136 Free PMC article.
-
An association between time-varying serum alkaline phosphatase concentrations and mortality rate in patients undergoing peritoneal dialysis: a five-year cohort study.Sci Rep. 2017 Mar 3;7:43314. doi: 10.1038/srep43314. Sci Rep. 2017. PMID: 28256582 Free PMC article.
-
Beyond Numbers: How Biochemical Parameters Can Predict Outcomes in Chronic Kidney Disease Patients on Maintenance Hemodialysis.Cureus. 2024 Aug 20;16(8):e67349. doi: 10.7759/cureus.67349. eCollection 2024 Aug. Cureus. 2024. PMID: 39310569 Free PMC article.
-
Diagnostic Workup for Disorders of Bone and Mineral Metabolism in Patients with Chronic Kidney Disease in the Era of KDIGO Guidelines.Int J Nephrol. 2011;2011:958798. doi: 10.4061/2011/958798. Epub 2011 Apr 7. Int J Nephrol. 2011. PMID: 21603118 Free PMC article.
References
-
- Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol. 2004;15:2208–2218. - PubMed
-
- Kalantar-Zadeh K, Kuwae N, Regidor DL, et al. Survival predictability of time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006;70:771–780. - PubMed
-
- Kovesdy CP, Kalantar-Zadeh K. Bone and mineral disorders in pre-dialysis CKD. Int Urol Nephrol. 2008;40:427–440. - PubMed
-
- Kestenbaum B, Sampson JN, Rudser KD, et al. Serum phosphate levels and mortality risk among people with chronic kidney disease. J Am Soc Nephrol. 2005;16:520–528. - PubMed
-
- Voormolen N, Noordzij M, Grootendorst DC, et al. High plasma phosphate as a risk factor for decline in renal function and mortality in pre-dialysis patients. Nephrol Dial Transplant. 2007;22:2909–2916. - PubMed
