

JC virus infection of the brain
- PMID: 20299430
- PMCID: PMC7965014
- DOI: 10.3174/ajnr.A2035
JC virus infection of the brain
Abstract
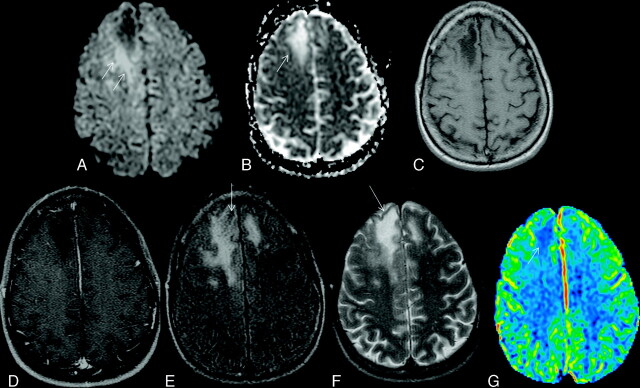
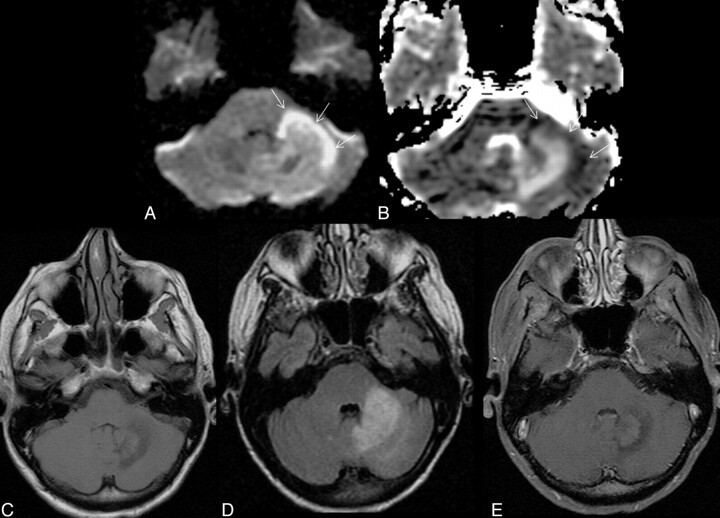
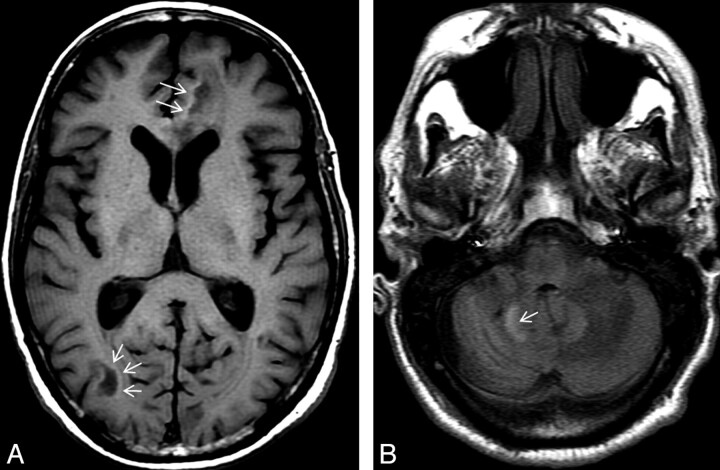
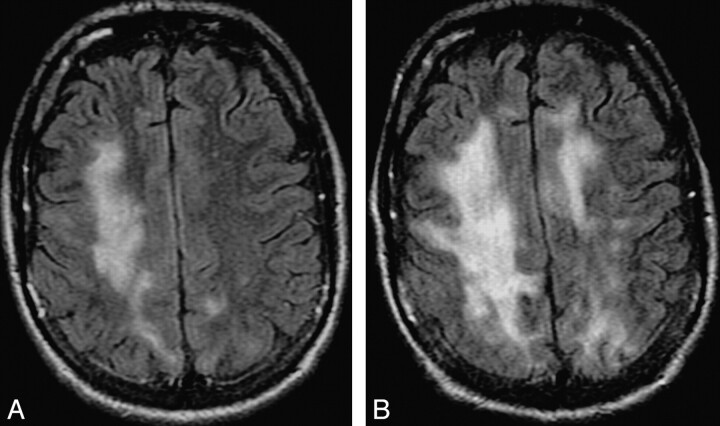
Since its initial description, there have been significant changes in the epidemiology, pathogenesis, and clinical and imaging manifestations of JCV infection of brain. The most common clinical manifestation is PML. Other recently described CNS manifestations are JCE, JCVGCN, and JCM. Although AIDS is the most common predisposing factor for JCV reactivation, there is increasing incidence of brain manifestations of JCV reactivation in non-HIV settings, including different rheumatologic, hematologic, and oncologic conditions; monoclonal antibody therapy; transplant recipients; primary immunodeficiency syndromes; and even in patients without any recognizable immune deficiency. IRIS may develop secondary to restoration of immunity in HIV-positive patients with PML receiving antiretroviral therapy. This is of profound clinical significance and needs to be diagnosed promptly. Imaging plays a crucial role in the diagnosis of the disease, monitoring of treatment response, identifying disease progression, and predicting prognosis. In this article, current understanding of the epidemiology, pathogenesis, clinical presentations, and all aspects of imaging of JCV infection of the brain have been comprehensively reviewed.
Figures
Comment in
-
Proton MR spectroscopy of progressive multifocal leukoencephalopathy-immune reconstitution inflammatory syndrome.AJNR Am J Neuroradiol. 2010 Sep;31(8):E69-70; author reply E71. doi: 10.3174/ajnr.A2160. Epub 2010 Jun 10. AJNR Am J Neuroradiol. 2010. PMID: 20538829 Free PMC article. No abstract available.
References
-
- Padgett BL, Walker DL, Zu Rhein GM, et al. . Cultivation of papova-like virus from human brain with progressive multifocal leucoencephalopathy. Lancet 1971; 29: 1257– 60 - PubMed
-
- Åström KE, Mancall EL, Richardson EP. Progressive multifocal leuko-encephalopathy: a hitherto unrecognized complication of chronic lymphatic leukaemia and Hodgkin's disease. Brain 1958; 81: 93– 111 - PubMed
-
- Hartman EA, Huang D. Update on PML: lessons from the HIV uninfected and new insights in pathogenesis and treatment. Curr Hiv/AIDS Rep 2008; 5: 112– 19 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical