

Artery of percheron infarction: imaging patterns and clinical spectrum
- PMID: 20299438
- PMCID: PMC7965474
- DOI: 10.3174/ajnr.A2044
Artery of percheron infarction: imaging patterns and clinical spectrum
Abstract
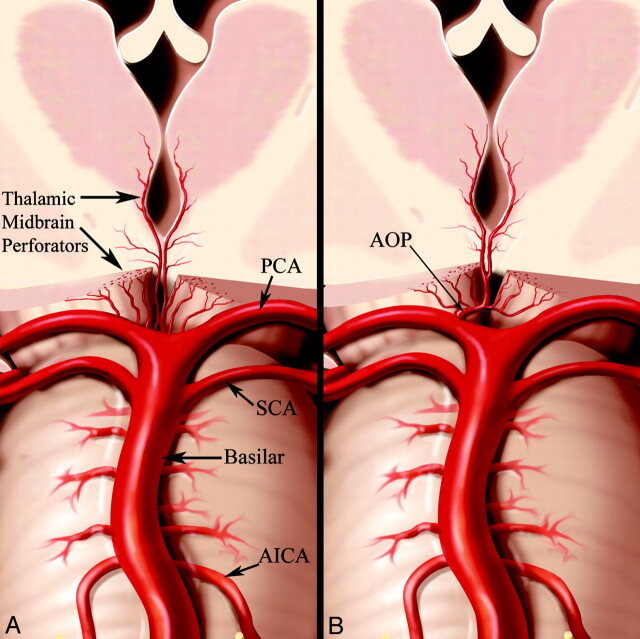
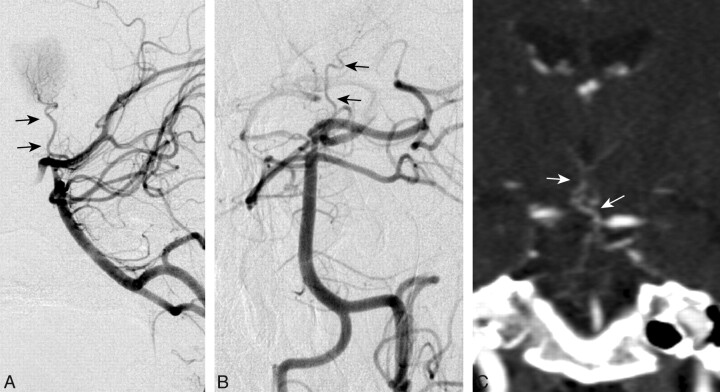
Background and purpose: Occlusion of the AOP results in a characteristic pattern of ischemia: bilateral paramedian thalamus with or without midbrain involvement. Although the classic imaging findings are often recognized, only a few small case series and isolated cases of AOP infarction have been reported. The purpose of this study was to characterize the complete imaging spectrum of AOP infarction on the basis of a large series of cases obtained from multiple institutions.
Materials and methods: Imaging and clinical data of 37 patients with AOP infarction from 2000 to 2009 were reviewed retrospectively. The primary imaging criterion for inclusion was an abnormal signal intensity on MR imaging and/or hypoattenuation on CT involving distinct arterial zones of the bilateral paramedian thalami with or without rostral midbrain involvement. Patients were excluded if there was a neoplastic, infectious, or inflammatory etiology.
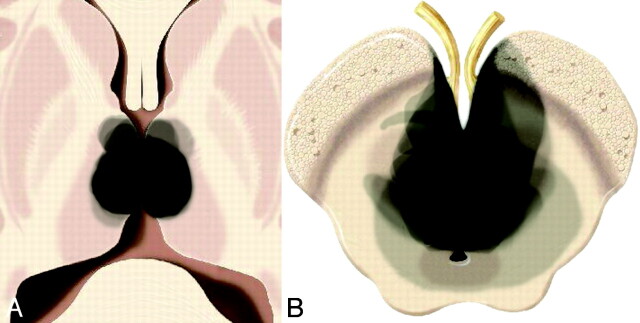
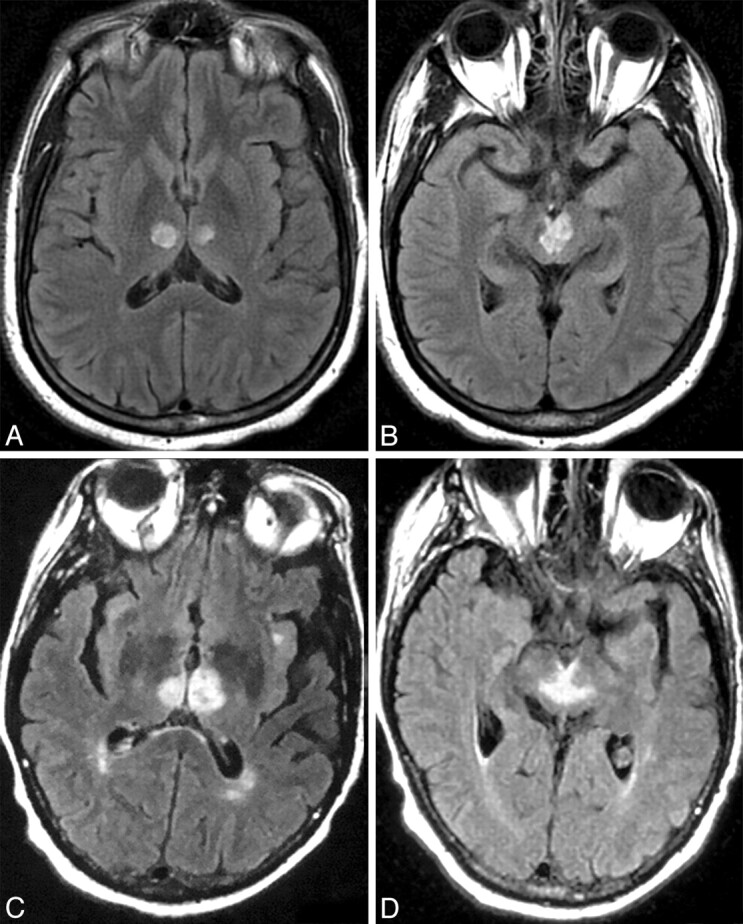
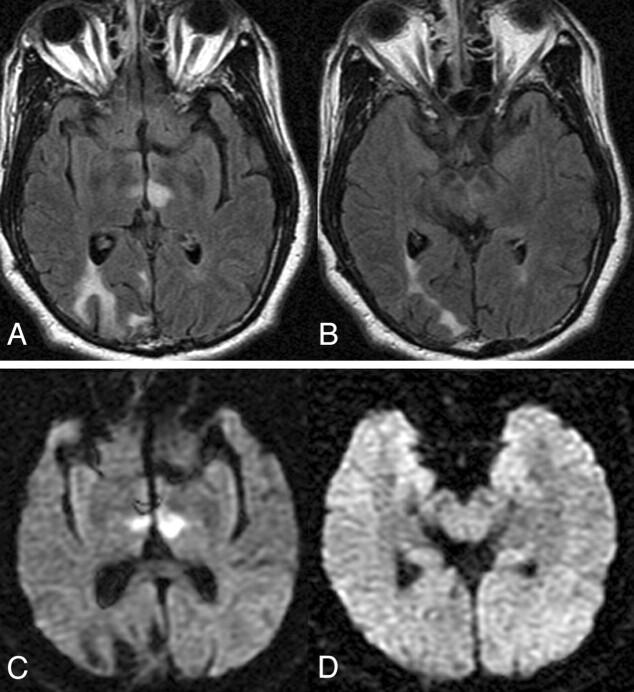
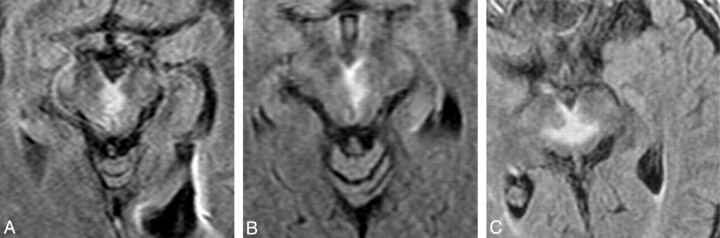
Results: We identified 4 ischemic patterns of AOP infarction: 1) bilateral paramedian thalamic with midbrain (43%), 2) bilateral paramedian thalamic without midbrain (38%), 3) bilateral paramedian thalamic with anterior thalamus and midbrain (14%), and 4) bilateral paramedian thalamic with anterior thalamus without midbrain (5%). A previously unreported finding (the "V" sign) on FLAIR and DWI sequences was identified in 67% of cases of AOP infarction with midbrain involvement and supports the diagnosis when present.
Conclusions: The 4 distinct patterns of ischemia identified in our large case series, along with the midbrain V sign, should improve recognition of AOP infarction and assist with the neurologic evaluation and management of patients with thalamic strokes.
Figures
References
-
- Castaigne P, Lhermitte F, Buge A, et al. . Paramedian thalamic and midbrain infarct: clinical and neuropathological study. Ann Neurol 1981;10:127–48 - PubMed
-
- Carrera E, Michel P, Bogousslavsky J. Anteromedian, central, and posterolateral infarcts of the thalamus: three variant types. Stroke 2004;35:2826–31 - PubMed
-
- Takahashi S, Suzuki M, Matsumoto K, et al. . Extent and location of cerebral infarcts on multiplanar MR images: correlation with distribution of perforating arteries on cerebral angiograms and on cadaveric microangiograms. AJR Am J Roentgenol 1994;163:1215–22 - PubMed
-
- Bogousslavsky J, Regli F, Uske A. Thalamic infarcts: clinical syndromes, etiology, and prognosis. Neurology 1988;38:837–48 - PubMed
-
- Kumral E, Evyapan D, Balkir K, et al. . Bilateral thalamic infarction: clinical, etiological and MRI correlates. Acta Neurol Scand 2001;103:35–42 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical