

Long-term cognitive and psychological outcomes in the awakening and breathing controlled trial
- PMID: 20299535
- PMCID: PMC2913233
- DOI: 10.1164/rccm.200903-0442OC
Long-term cognitive and psychological outcomes in the awakening and breathing controlled trial
Abstract
Rationale: Studies have shown that reducing sedation of critically ill patients shortens time on the ventilator and in the intensive care unit (ICU). Little is known, however, of how such strategies affect long-term cognitive, psychological, and functional outcomes.
Objectives: To determine the long-term effects of a wake up and breathe protocol that interrupts and reduces sedative exposure in the ICU.
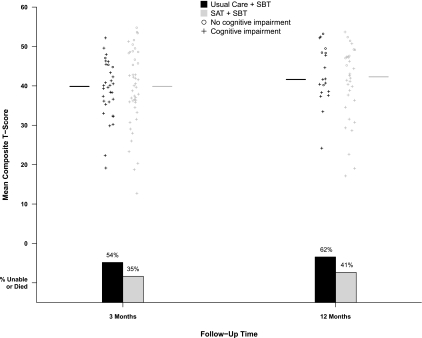
Methods: In this a priori planned substudy conducted at one tertiary care hospital during the Awakening and Breathing Controlled Trial, a multicenter randomized controlled trial, we assessed cognitive, psychological, and functional/quality-of-life outcomes 3 and 12 months postdischarge among 180 medical ICU patients randomized to paired daily spontaneous awakening trials with spontaneous breathing trials (SBTs) or to sedation per usual care plus daily SBTs.
Measurements and main results: Cognitive impairment was less common in the intervention group at 3-month follow-up (absolute risk reduction, 20.2%; 95% confidence interval, 1.5-36.1%; P = 0.03) but not at 12-month follow-up (absolute risk reduction, -1.9%; 95% CI, -21.3 to 27.1%; P = 0.89). Composite cognitive scores, alternatively, were similar in the two groups at 3-month and 12-month follow-up (P = 0.80 and 0.61, respectively), as were symptoms of depression (P = 0.59 and 0.82) and posttraumatic stress disorder (P = 0.59 and 0.97). Activities of daily living, functional status, and mental and physical quality of life were similar between groups throughout follow-up.
Conclusions: In this trial, management of mechanically ventilated medical ICU patients with a wake up and breathe protocol resulted in similar cognitive, psychological, and functional outcomes among patients tested 3 and 12 months post-ICU. The proven benefits of this protocol, including improved 1-year survival, were not offset by adverse long-term outcomes. Clinical trial registered with www.clinicaltrials.gov (NCT 00097630).
Trial registration: ClinicalTrials.gov NCT00097630.
Figures

References
-
- Arroliga AC, Thompson BT, Ancukiewicz M, Gonzales JP, Guntupalli KK, Park PK, Wiedemann HP, Anzueto A. Use of sedatives, opioids, and neuromuscular blocking agents in patients with acute lung injury and acute respiratory distress syndrome. Crit Care Med 2008;36:1083–1088. - PubMed
-
- Weinert CR, Calvin AD. Epidemiology of sedation and sedation adequacy for mechanically ventilated patients in a medical and surgical intensive care unit. Crit Care Med 2007;35:393–401. - PubMed
-
- Payen JF, Chanques G, Mantz J, Hercule C, Auriant I, Leguillou JL, Binhas M, Genty C, Rolland C, Bosson JL. Current practices in sedation and analgesia for mechanically ventilated critically ill patients: a prospective multicenter patient-based study. Anesthesiology 2007;106:687–695. - PubMed
-
- Heffner JE. A wake-up call in the intensive care unit. N Engl J Med 2000;342:1520–1522. - PubMed
-
- Brochard L. Sedation in the intensive-care unit: good and bad? Lancet 2008;371:95–97. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
