

Tetralogy of Fallot: Current surgical perspective
- PMID: 20300249
- PMCID: PMC2840758
- DOI: 10.4103/0974-2069.43873
Tetralogy of Fallot: Current surgical perspective
Abstract
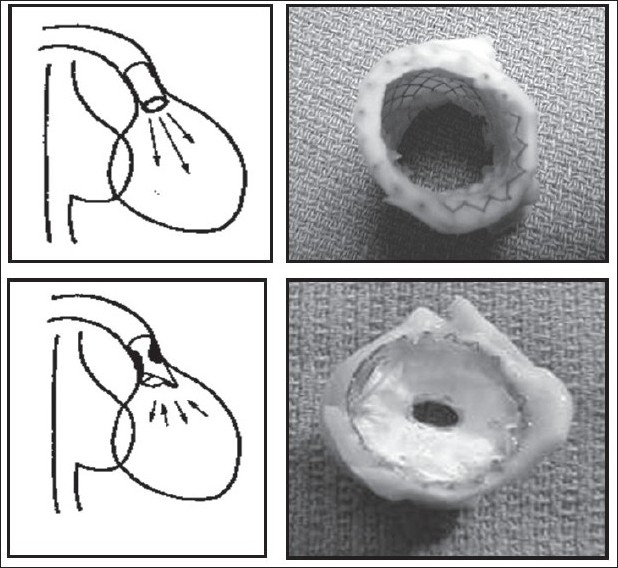
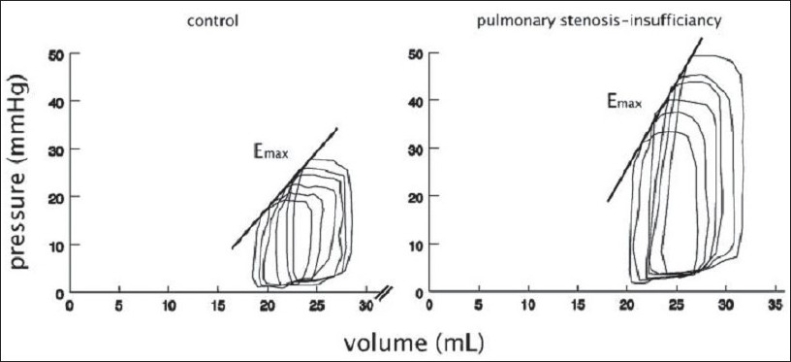
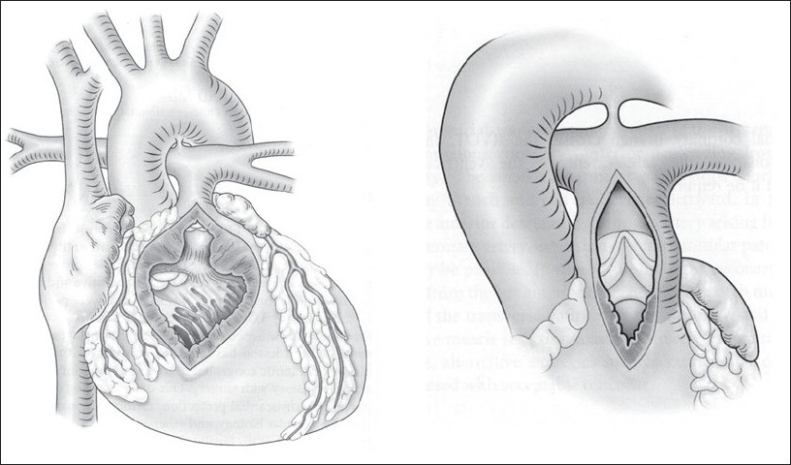
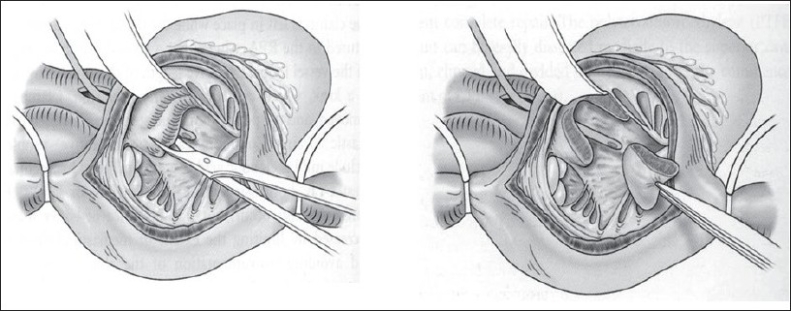
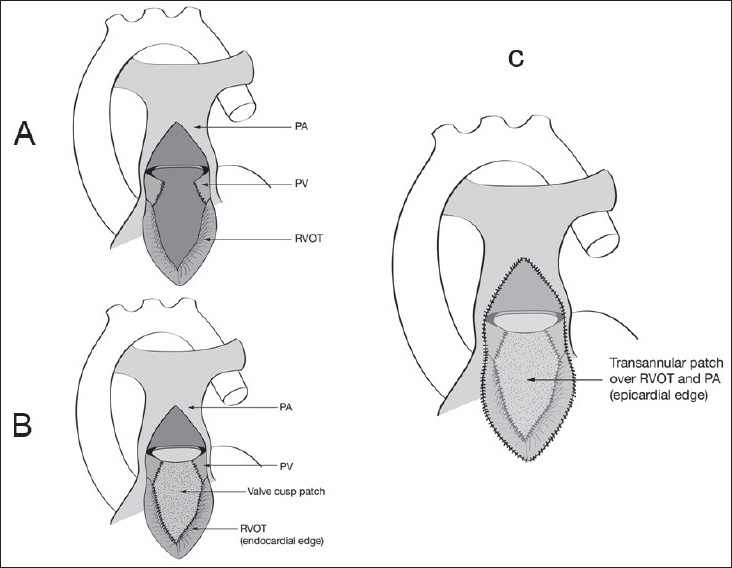
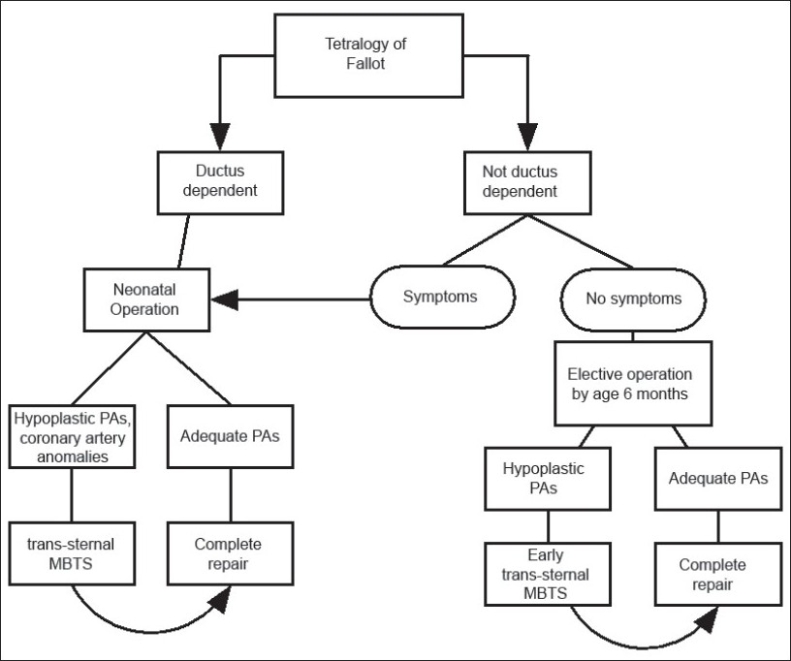
Tetralogy of Fallot (TOF) is an important lesion for all pediatric and congenital heart surgeons. In designing the most appropriate operation for children with TOF, the postoperative physiology should be taken into account, both in the short and long term. The balance between pulmonary stenosis (PS) and pulmonary insufficiency (PI) may be critical for preservation of ventricular function. A unified repair strategy that limits both residual PS and PI is presented, along with supporting experimental evidence, a strategy for dealing with coronary anomalies, and comments regarding best timing of operation.
Keywords: Right ventricular function; residual pulmonary incompetence; residual right ventricular outflow obstruction.
Conflict of interest statement
Figures
References
-
- Knott-Craig CJ, Elkins RC, Lane MM, Holz J, McCue C, Ward KE. A 26-year experience with surgical management of tetralogy of Fallot: Risk analysis for mortality or late reintervention. Ann Thorac Surg. 1998;66:506–11. - PubMed
-
- Nollert G, Fischlein T, Bouterwek S, Böhmer C, Klinner W, Reichart B. Long-term survival in patients with repair of tetralogy of Fallot: 36-year follow-up of 490 survivors of the first year after surgical repair. J Am Coll Cardiol. 1997;30:1374–83. - PubMed
-
- Kilner PJ, Balossino R, Dubini G, Babu-Narayan SV, Taylor AM, Pennati G, et al. Pulmonary regurgitation: The effects of varying pulmonary artery compliance, and of increased resistance proximal or distal to the compliance. Int J Cardiol. 2008 Aug 20; [Epub ahead of print] - PubMed
-
- Hon J, Steendijk P, Khan H, Wong K, Yacoub M. Acute effects of pulmonary artery banding in sheep on right ventricle pressure-volume relations: Relevance to the arterial switch operation. Acta Physiol Scand. 2001;172:97–106. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
