

doi: 10.4103/0974-2069.52803.
Sequential segmental analysis
Affiliations
- PMID: 20300266
- PMCID: PMC2840778
- DOI: 10.4103/0974-2069.52803
Item in Clipboard
Sequential segmental analysis
Ann Pediatr Cardiol.
2009 Jan.
No abstract available
Conflict of interest statement
Figures
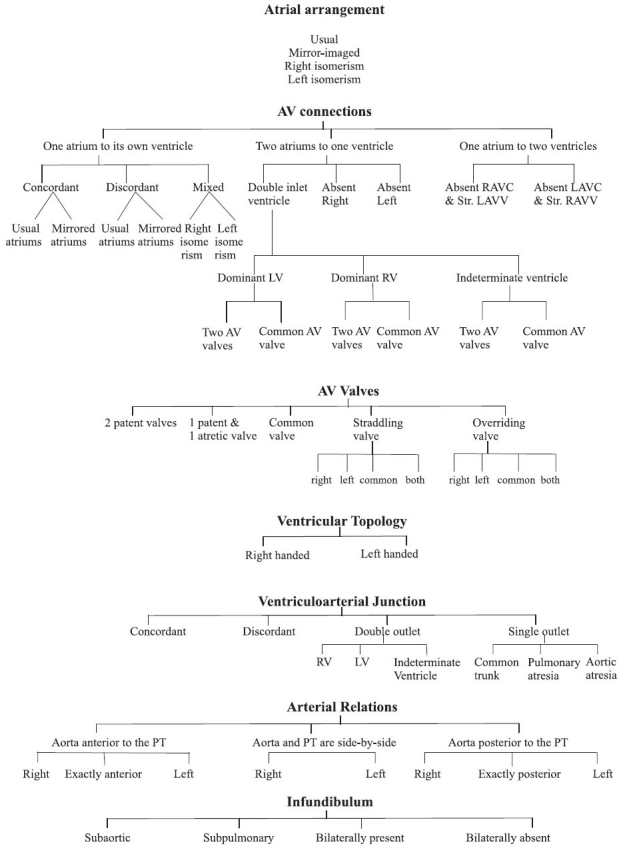
Variable features in sequential segmental analysis
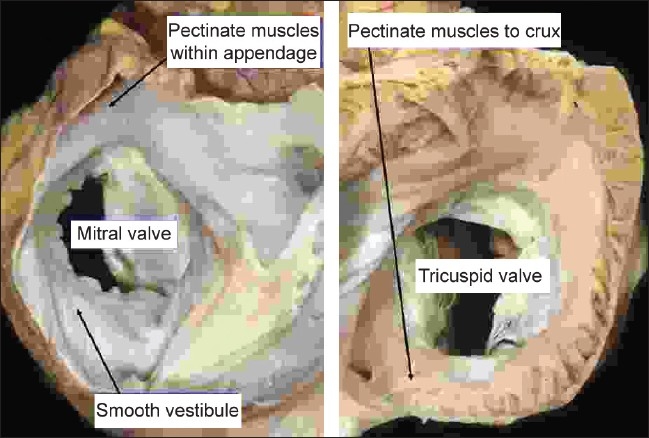
The images show the short axis views of the left (left hand panel) and right (right hand panel) atrioventricular junctions of the normal heart as seen from above, having opened the atriums with a cut parallel to the atrioventricular junctions. They show how, in the morphologically right atrium (right hand panel), the pectinate muscles within the the appendage extend all round the vestibule of the tricuspid valve. In the morphologically left atrium, in contrast (left hand panel), the pectinate muscles are confined within the tubular appendage, so that the inferior wall of the atrium is smooth
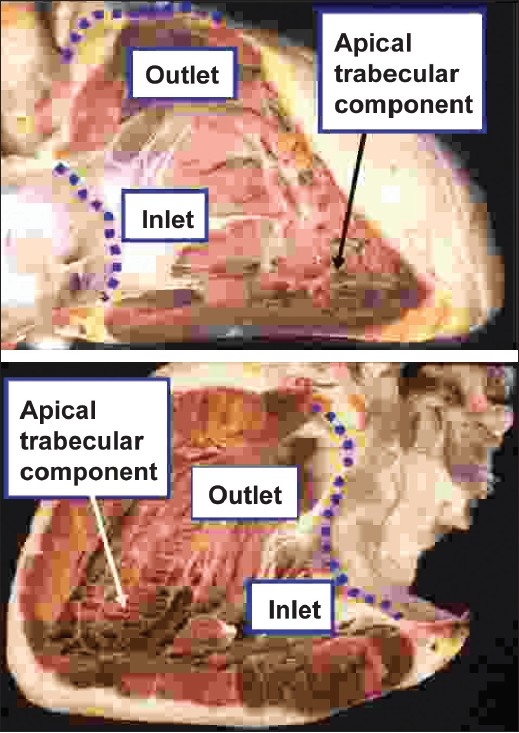
The upper panel shows the morphologically right ventricle, which extends from the atrioventricular to the ventriculo-arterial junctions (dotted red lines), with the anterior wall removed to show its three component parts. The coarse apical trabeculations are the most constant of these features. The lower panel shows the comparable three component parts of the morphologically left ventricle of the same heart, revealed by removing its posterior wall. This ventricle also extends from the atrioventricular to the ventriculo-arterial junctions (dotted purple lines). Its fine apical trabeculations are its most constant feature, and distinguish it from the morphologically right ventricle
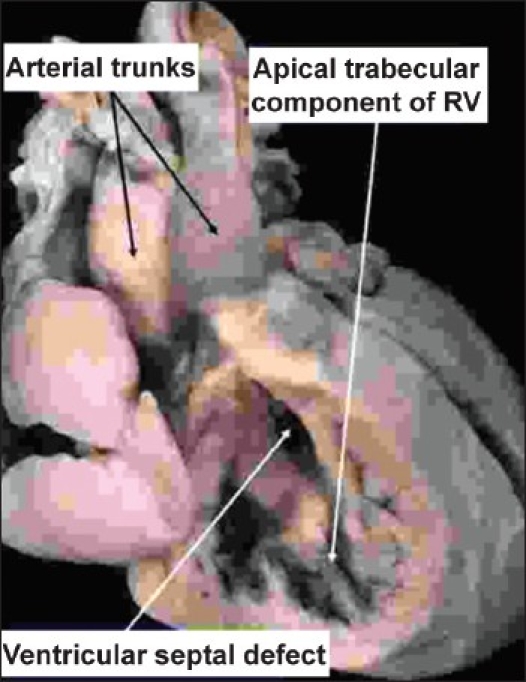
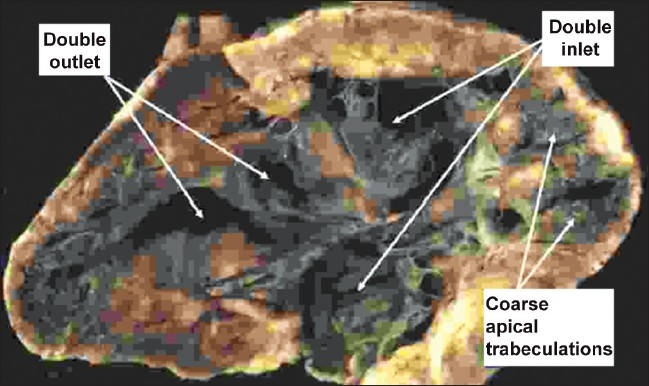
In the heart illustrated, there is double inlet to, and double outlet from a dominant left ventricle. The arterial trunks are seen arising in parallel fashion from the left ventricle, with the aorta anterior and to the left. On the anterior and right-sided shoulder of the dominant left ventricle, however, there is still a second chamber to be seen, fed through a ventricular septal defect. This chamber is the apical trabecular component of the right ventricle (RV), identified because of its coarse trabeculations
The heart is opened in clamshell fashion to show that both atrioventricular valves enter the same ventricular chamber, which also gives rise to both outflow tracts. We were unable to find a second ventricular chamber. The exceedingly coarse apical trabeculations, and the absence of the second chamber, identify this heart as having a solitary ventricle of indeterminate morphology
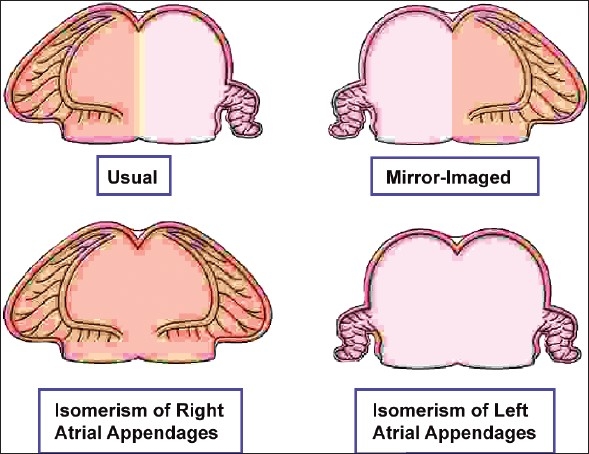
The cartoon shows how, when analysed on the basis of the extent of the pectinate muscles relative to the atrioventricular vestibules, there are only four possible ways for arrangement of two atrial appendages
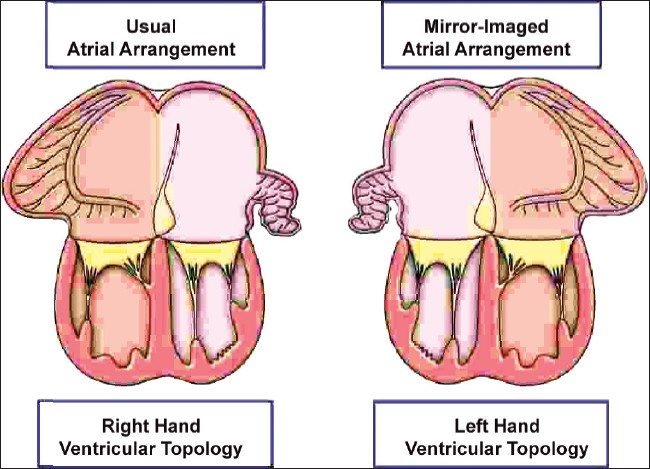
The cartoon shows how concordant atrioventricular connections can exist is usual and mirror-imaged patterns. Almost without exception, atriums with usually arranged appendages are joined to a ventricular mass with right hand topology, whilst atriums with mirror-imaged appendages are joined to a ventricular mass with left hand topology. Except when these associations are not present, it is not necessary also to state the topology of the ventricles
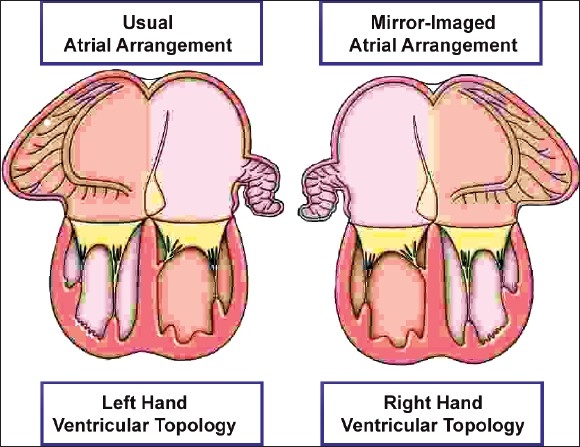
In this cartoon, the arrangements are shown that produce, almost without exception, discordant atrioventricular connections
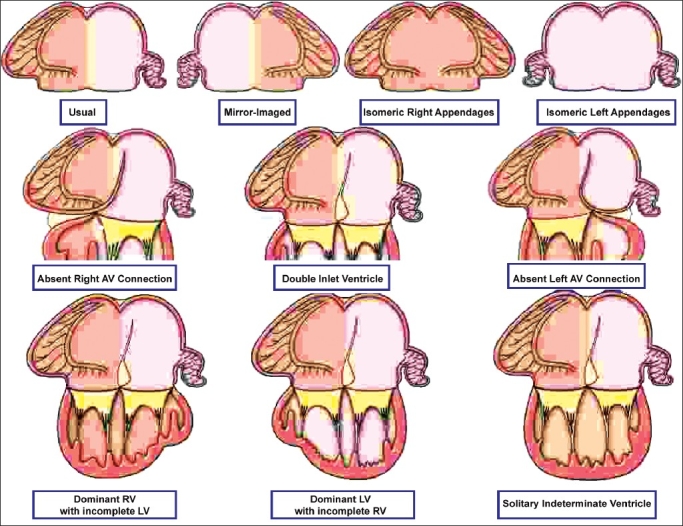
The cartoon shows some of the potential univentricular atrioventricular connections. In reality, these can exist with any arrangement of the atrial appendages (upper row), with double inlet, absent right, or absent left atrioventricular connections (middle row), and with dominant left or right ventricles, or solitary and indeterminate ventricle (bottom row). The possibilities are illustrated with usual arrangement of the atrial appendages simply for convenience, while the examples in the bottom row are shown only for double inlet ventricle. The same variation in ventricular morphology exists for hearts with absence of one atrioventricular connection. There is further variability with regard to the position of the incomplete ventricle, and with ventriculo-arterial connections, and so on. These hearts, therefore, exemplify the need for full sequential segmental analysis and description
References
-
- Van Praagh R. The segmental approach to diagnosis in congenital heart disease. In: Bergsma D, editor. Birth defects original article series, VIII, No. 5. The National Foundation – March of Dimes. Baltimore: Williams and Wilkins; 1972. pp. 4–23.
-
- Jacobs JP, Franklin RC, Colan SD, Jacobs ML, Tchervenkov CL, Maruszewski B, et al. Classification of the functionally univentricular heart: Unity from mapped codes. Cardiol Young. 2006;16:9–21. - PubMed
-
- de la Cruz MV, Nadal-Ginard B. Rules for the diagnosis of visceral situs, truncoconal morphologies, and ventricular inversions. Am Heart J. 1972;84:19–32. - PubMed
