

Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease
- PMID: 20301112
- PMCID: PMC2922495
- DOI: 10.1002/hep.23535
Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease
Abstract
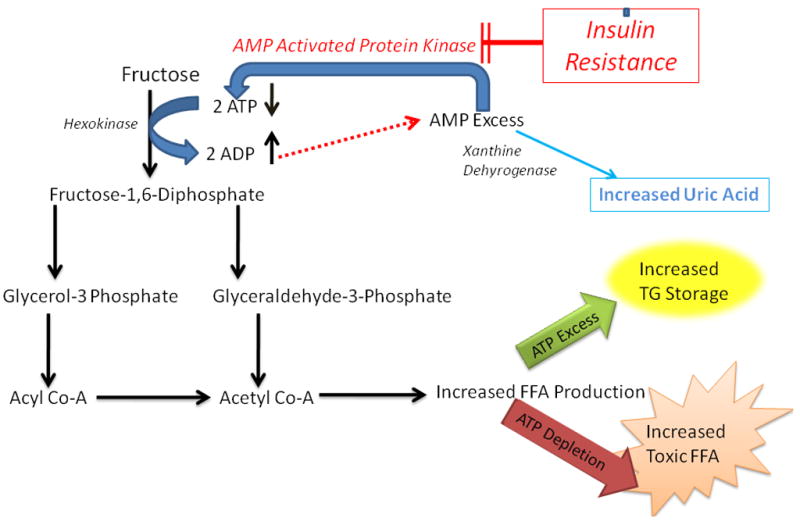
The rising incidence of obesity and diabetes coincides with a marked increase in fructose consumption. Fructose consumption is higher in individuals with nonalcoholic fatty liver disease (NAFLD) than in age-matched and body mass index (BMI)-matched controls. Because fructose elicits metabolic perturbations that may be hepatotoxic, we investigated the relationship between fructose consumption and disease severity in NAFLD. We studied 427 adults enrolled in the NASH Clinical Research Network for whom Block food questionnaire data were collected within 3 months of a liver biopsy. Fructose consumption was estimated based on reporting (frequency x amount) of Kool-aid, fruit juices, and nondietary soda intake, expressed as servings per week, and classified into none, minimum to moderate (<7 servings/week), and daily (> or =7 servings/week). The association of fructose intake with metabolic and histological features of NAFLD was analyzed using multiple linear and ordinal logistic regression analyses with and without controlling for other confounding factors. Increased fructose consumption was univariately associated with decreased age (P < 0.0001), male sex (P < 0.0001), hypertriglyceridemia (P < 0.04), low high-density lipoprotein (HDL) cholesterol (<0.0001), decreased serum glucose (P < 0.001), increased calorie intake (P < 0.0001), and hyperuricemia (P < 0.0001). After controlling for age, sex, BMI, and total calorie intake, daily fructose consumption was associated with lower steatosis grade and higher fibrosis stage (P < 0.05 for each). In older adults (age > or = 48 years), daily fructose consumption was associated with increased hepatic inflammation (P < 0.05) and hepatocyte ballooning (P = 0.05).
Conclusion: In patients with NAFLD, daily fructose ingestion is associated with reduced hepatic steatosis but increased fibrosis. These results identify a readily modifiable environmental risk factor that may ameliorate disease progression in patients with NAFLD.
Figures
Comment in
-
Non-alcoholic fatty liver disease and fructose: bad for us, better for mice.J Hepatol. 2011 Jul;55(1):218-20. doi: 10.1016/j.jhep.2011.01.029. Epub 2011 Feb 19. J Hepatol. 2011. PMID: 21338637 Free PMC article. No abstract available.
-
Two solutions in search of a problem.Hepatology. 2011 Jun;53(6):2148. doi: 10.1002/hep.24134. Epub 2011 Apr 6. Hepatology. 2011. PMID: 21472743 No abstract available.
References
-
- Collison KS, Saleh SM, Bakheet RH, Al-Rabiah RK, Inglis AL, Makhoul NJ, Maqbool ZM, et al. Diabetes of the Liver: The Link Between Nonalcoholic Fatty Liver Disease and HFCS-55. Obesity (Silver Spring) 2009 - PubMed
-
- Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. Am J Gastroenterol. 2003;98:960–967. - PubMed
-
- Lazo M, Clark JM. The epidemiology of nonalcoholic fatty liver disease: a global perspective. Semin Liver Dis. 2008;28:339–350. - PubMed
-
- Elliott SS, Keim NL, Stern JS, Teff K, Havel PJ. Fructose, weight gain, and the insulin resistance syndrome. Am J Clin Nutr. 2002;76:911–922. - PubMed
-
- Bray GA, Nielsen SJ, Popkin BM. Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity. Am J Clin Nutr. 2004;79:537–543. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1RR02501401/RR/NCRR NIH HHS/United States
- U01DK061713/DK/NIDDK NIH HHS/United States
- U01 DK061732/DK/NIDDK NIH HHS/United States
- U01DK061731/DK/NIDDK NIH HHS/United States
- U01DK061737/DK/NIDDK NIH HHS/United States
- UL1RR02413101/RR/NCRR NIH HHS/United States
- M01RR000065/RR/NCRR NIH HHS/United States
- U01DK061718/DK/NIDDK NIH HHS/United States
- U01DK061732/DK/NIDDK NIH HHS/United States
- U01DK061728/DK/NIDDK NIH HHS/United States
- U01 DK061730/DK/NIDDK NIH HHS/United States
- K23 DK062116/DK/NIDDK NIH HHS/United States
- UL1RR024989/RR/NCRR NIH HHS/United States
- M01RR020359/RR/NCRR NIH HHS/United States
- M01RR000827/RR/NCRR NIH HHS/United States
- U01DK061738/DK/NIDDK NIH HHS/United States
- I01 BX002586/BX/BLRD VA/United States
- M01RR00188/RR/NCRR NIH HHS/United States
- U01DK061734/DK/NIDDK NIH HHS/United States
- U01DK061730/DK/NIDDK NIH HHS/United States
- M01RR000750/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical