

Blood still kills: six strategies to further reduce allogeneic blood transfusion-related mortality
- PMID: 20303034
- PMCID: PMC7126657
- DOI: 10.1016/j.tmrv.2009.11.001
Blood still kills: six strategies to further reduce allogeneic blood transfusion-related mortality
Erratum in
- Transfus Med Rev. 2010 Jul;24(3):257
Abstract
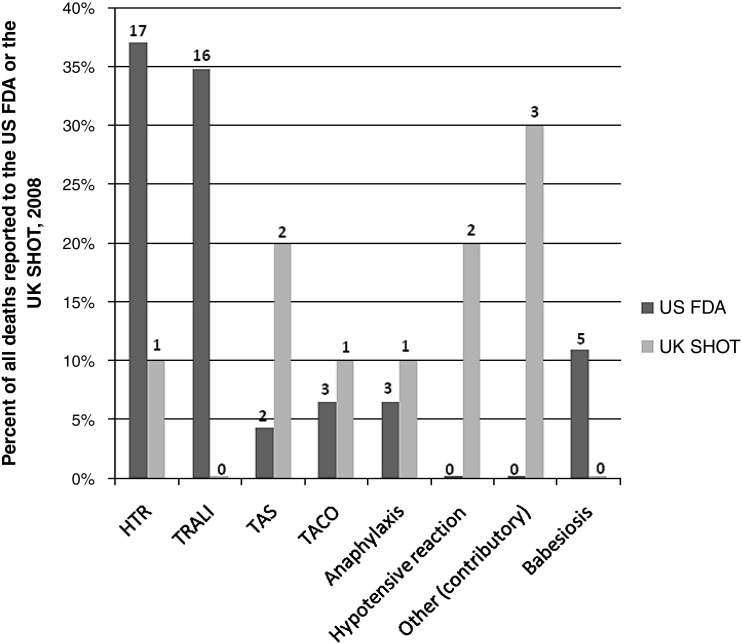
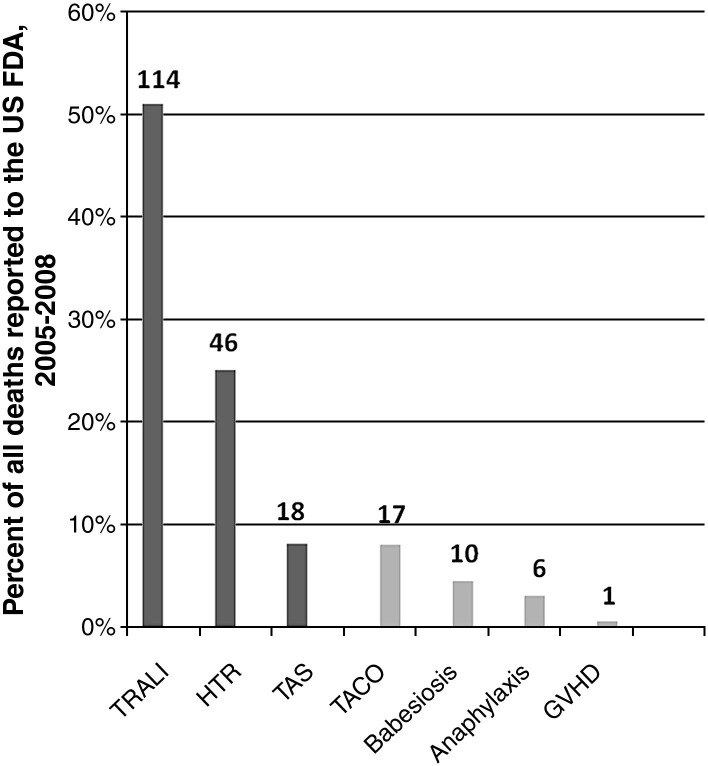
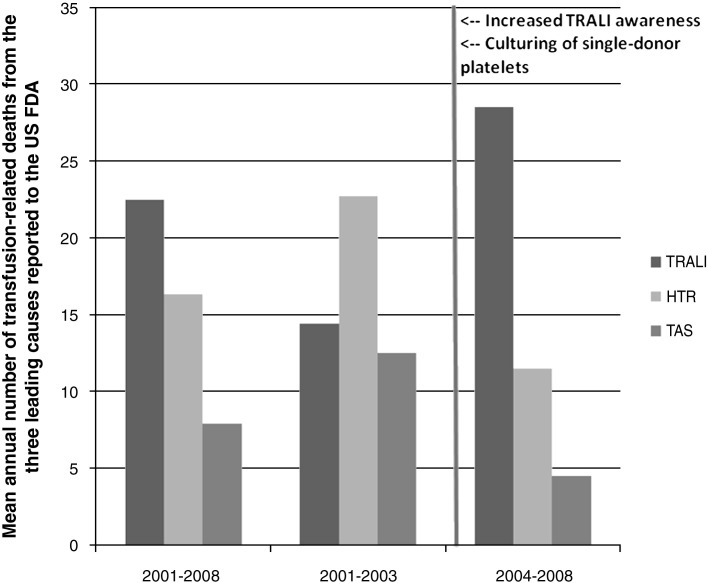
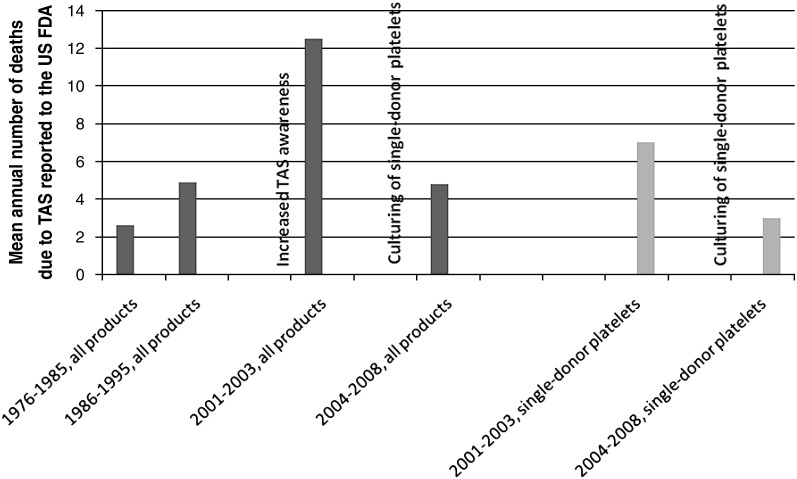
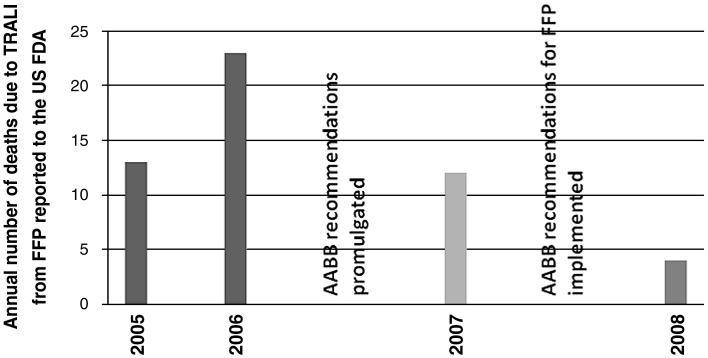
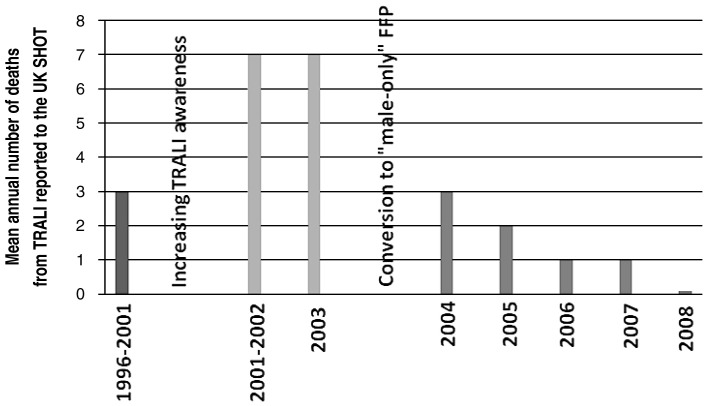
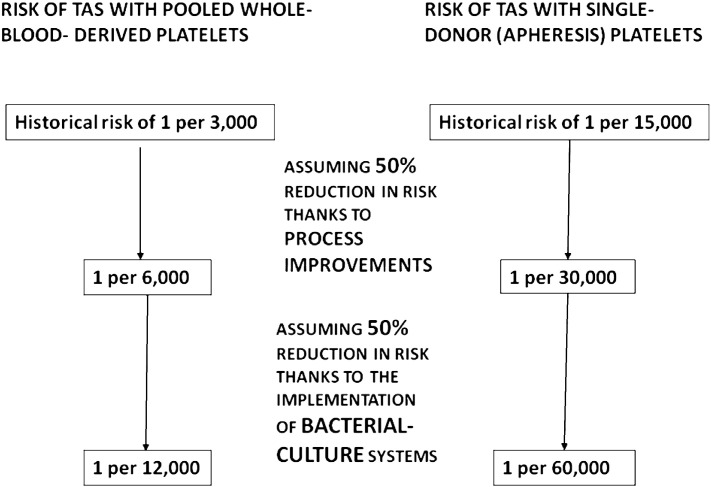
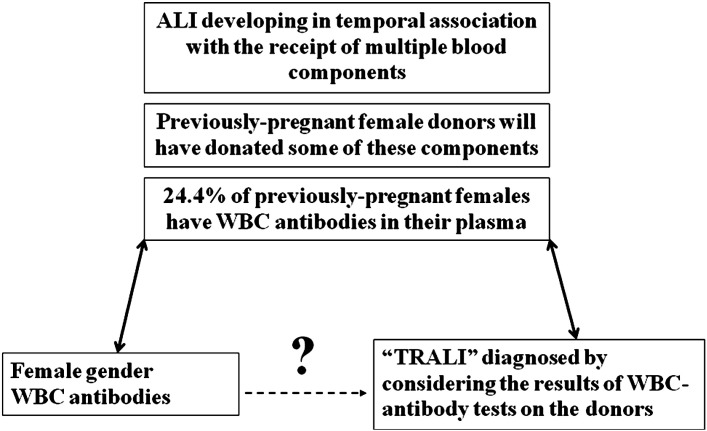
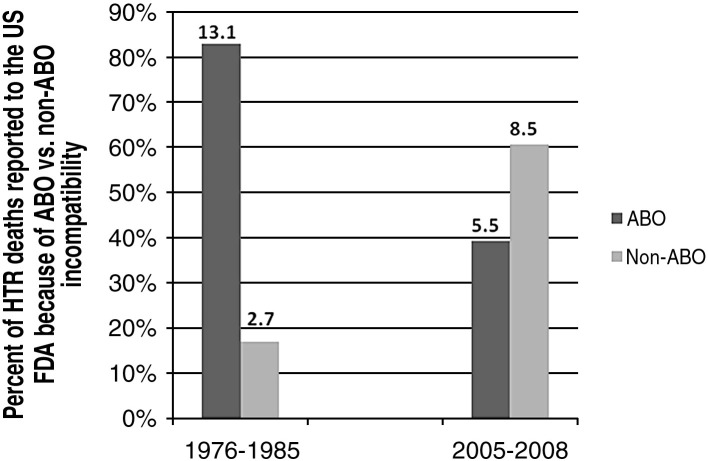
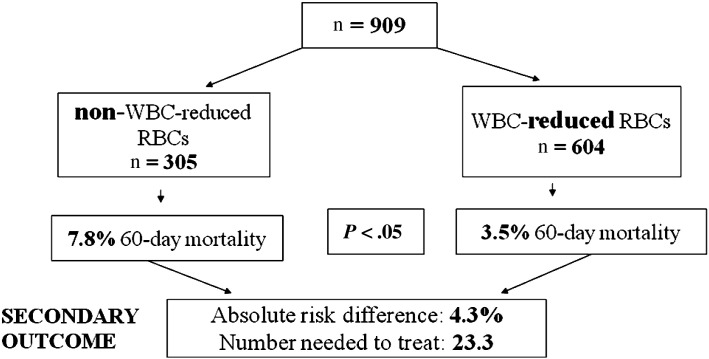
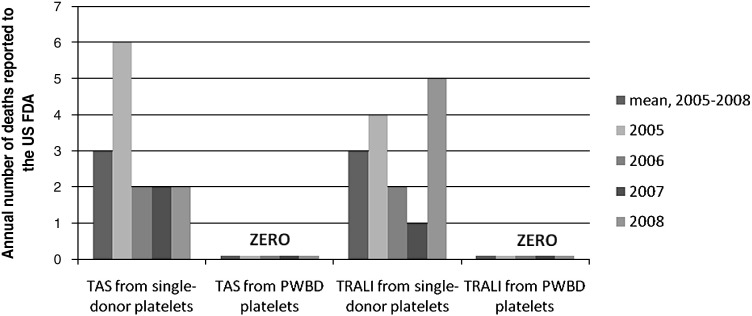
After reviewing the relative frequency of the causes of allogeneic blood transfusion-related mortality in the United States today, we present 6 possible strategies for further reducing such transfusion-related mortality. These are (1) avoidance of unnecessary transfusions through the use of evidence-based transfusion guidelines, to reduce potentially fatal (infectious as well as noninfectious) transfusion complications; (2) reduction in the risk of transfusion-related acute lung injury in recipients of platelet transfusions through the use of single-donor platelets collected from male donors, or female donors without a history of pregnancy or who have been shown not to have white blood cell (WBC) antibodies; (3) prevention of hemolytic transfusion reactions through the augmentation of patient identification procedures by the addition of information technologies, as well as through the prevention of additional red blood cell alloantibody formation in patients who are likely to need multiple transfusions in the future; (4) avoidance of pooled blood products (such as pooled whole blood-derived platelets) to reduce the risk of transmission of emerging transfusion-transmitted infections (TTIs) and the residual risk from known TTIs (especially transfusion-associated sepsis [TAS]); (5) WBC reduction of cellular blood components administered in cardiac surgery to prevent the poorly understood increased mortality seen in cardiac surgery patients in association with the receipt of non-WBC-reduced (compared with WBC-reduced) transfusion; and (6) pathogen reduction of platelet and plasma components to prevent the transfusion transmission of most emerging, potentially fatal TTIs and the residual risk of known TTIs (especially TAS).
(c) 2010 Elsevier Inc. All rights reserved.
Figures

References
-
- FDA/CBER: Fatalities reported to the FDA following blood collection and transfusion Annual summary for fiscal year 2008. http://www.fda.gov/cber/blood/SafetyAvailability/ReportaProblem/Transfus... Available at. Accessed September 21, 2009.
-
- Popovsky M.A., Moore S.B. Diagnostic and pathogenetic considerations in transfusion-related acute lung injury. Transfusion. 1985;25:573–577. - PubMed
-
- Goldman M., Blajchman M.A. Blood products-associated bacterial sepsis. Transfus Med Rev. 1991;5:73–83. - PubMed
-
- Sazama K. Reports of 355 transfusion-associated deaths: 1976 through 1985. Transfusion. 1990;30:583–590. - PubMed
-
- Popovsky M.A., Chaplin H.C., Jr., Moore S.B. Transfusion-related acute lung injury: A neglected, serious complication of hemotherapy. Transfusion. 1992;32:589–592. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
