

Dissociation between intrahepatic triglyceride content and insulin resistance in familial hypobetalipoproteinemia
- PMID: 20303351
- PMCID: PMC2902714
- DOI: 10.1053/j.gastro.2010.03.039
Dissociation between intrahepatic triglyceride content and insulin resistance in familial hypobetalipoproteinemia
Abstract
Background & aims: Hepatic steatosis is associated with insulin resistance, but it is not clear whether increased intrahepatic triglyceride (IHTG) content causes the resistance or is a marker. Subjects with familial hypobetalipoproteinemia (FHBL) have high levels of IHTG because of a genetic defect in hepatic export of triglycerides, and provide a unique cohort to study the relationship between steatosis and insulin sensitivity.
Methods: One group of lean subjects with normal IHTG content (2.2% +/- 0.6% of liver volume) (n = 6), and 3 groups of overweight and obese subjects matched for body mass index, were studied: (1) normal IHTG content (3.3% +/- 0.5%; n = 6), (2) high IHTG content (21.4% +/- 2.6%) due to nonalcoholic fatty liver disease (NAFLD; n = 6), and (3) high IHTG content (18.1% +/- 2.2%) due to FHBL (n = 3). A hyperinsulinemic-euglycemic clamp procedure, in conjunction with glucose tracer infusion, was used to determine multiorgan insulin sensitivity.
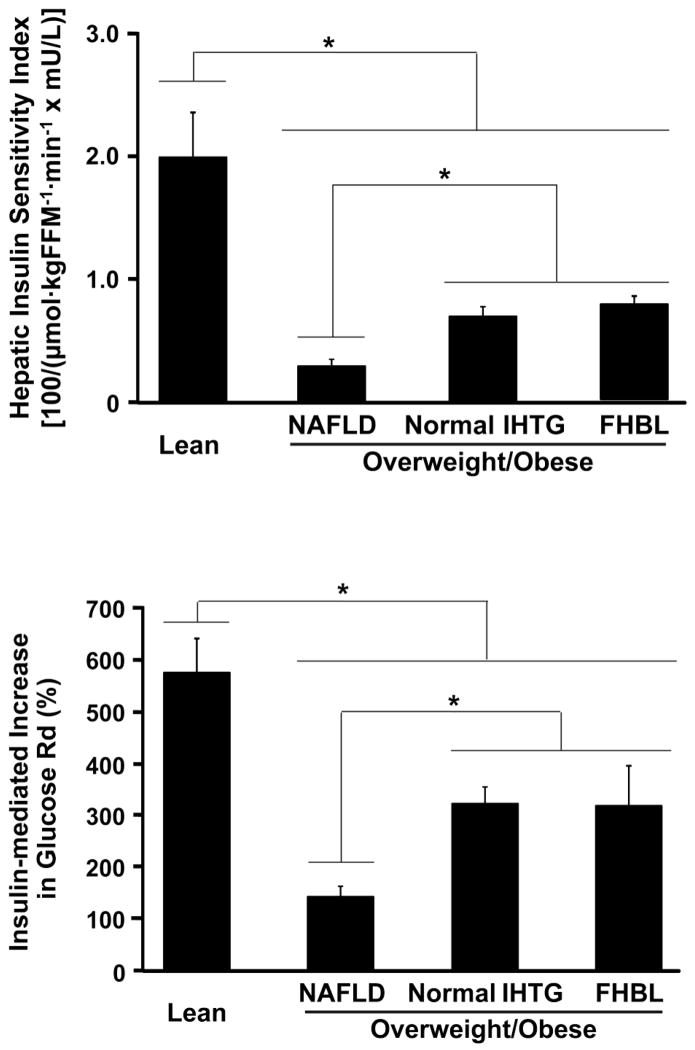
Results: Hepatic insulin sensitivity (reciprocal of glucose rate of appearance [micromol x kg fat-free mass(-1) x min(-1)] x insulin [mU/L]) was greatest in the Lean group (2.0 +/- 0.4); it was the same among subjects with FHBL (0.8 +/- 0.1) and the group with normal IHTG content, matched for body mass index (0.7 +/- 0.1), but greater than the NAFLD group (0.3 +/- 0.1) (P < .01). Muscle insulin sensitivity (percent increase in glucose uptake during insulin infusion) was greatest in the Lean group (576% +/- 70%). Muscle insulin sensitivity was similar in subjects with FHBL and those with normal IHTG (319% +/- 77%, 326% +/- 27%, respectively), but greater than the NAFLD group (145% +/- 18%) (P < .01).
Conclusions: Steatosis is dissociated from insulin resistance in FHBL, which suggests that increased IHTG content is a marker, not a cause, of metabolic dysfunction.
Copyright 2010 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Sanyal AJ, Campbell-Sargent C, Mirshahi F, Rizzo WB, Contos MJ, Sterling RK, et al. Nonalcoholic steatohepatitis: association of insulin resistance and mitochondrial abnormalities. Gastroenterology. 2001;120:1183–1192. - PubMed
-
- Seppala-Lindroos A, Vehkavaara S, Hakkinen AM, Goto T, Westerbacka J, Sovijarvi A, et al. Fat accumulation in the liver is associated with defects in insulin suppression of glucose production and serum free fatty acids independent of obesity in normal men. J Clin Endocrinol Metab. 2002;87:3023–3028. - PubMed
-
- Klein S, Mittendorfer B, Eagon JC, Patterson B, Grant L, Feirt N, et al. Gastric bypass surgery improves metabolic and hepatic abnormalities associated with nonalcoholic fatty liver disease. Gastroenterology. 2006;130:1564–1572. - PubMed
-
- Reeds DN, Yarasheski KE, Fontana L, Cade WT, Laciny E, DeMoss A, et al. Alterations in liver, muscle, and adipose tissue insulin sensitivity in men with HIV infection and dyslipidemia. Am J Physiol Endocrinol Metab. 2006;290:E47–E53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
