

Asbestos, carbon nanotubes and the pleural mesothelium: a review of the hypothesis regarding the role of long fibre retention in the parietal pleura, inflammation and mesothelioma
- PMID: 20307263
- PMCID: PMC2857820
- DOI: 10.1186/1743-8977-7-5
Asbestos, carbon nanotubes and the pleural mesothelium: a review of the hypothesis regarding the role of long fibre retention in the parietal pleura, inflammation and mesothelioma
Abstract
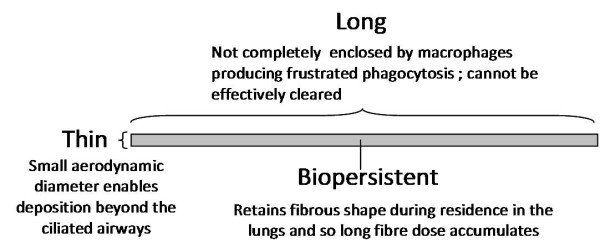
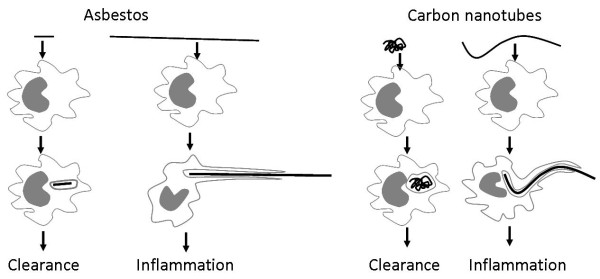
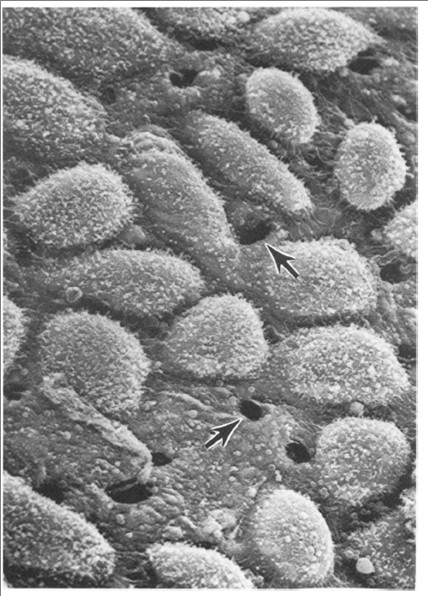
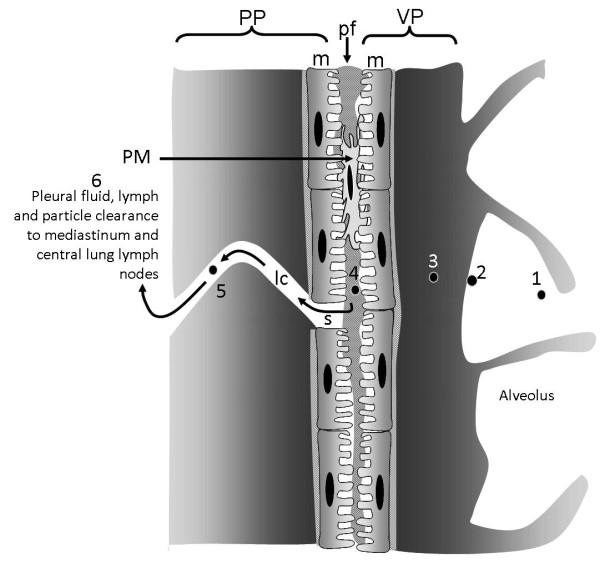
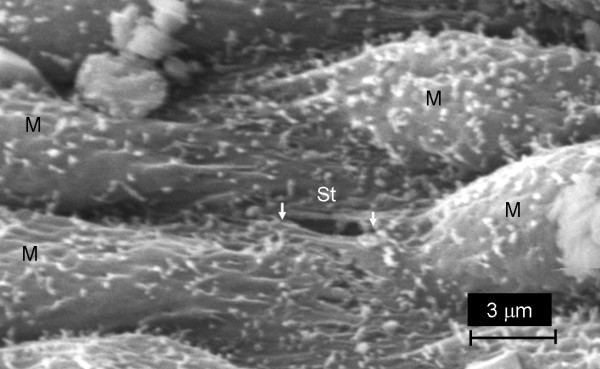
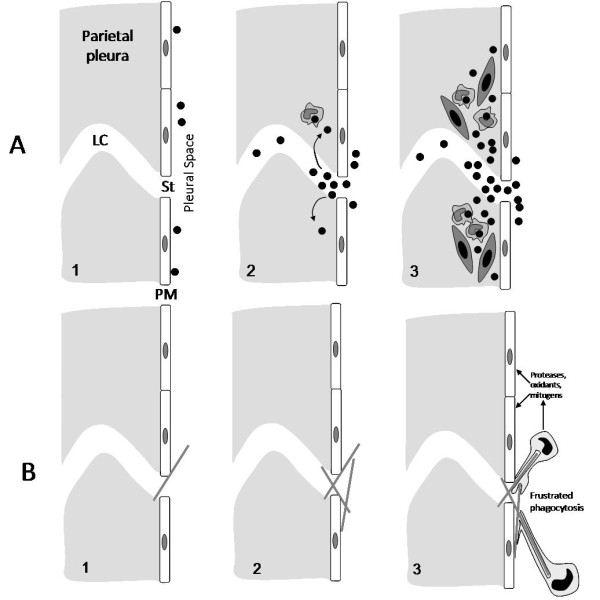
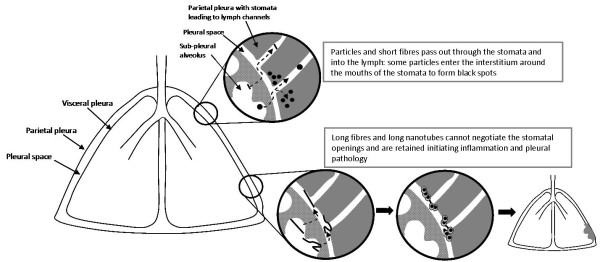
The unique hazard posed to the pleural mesothelium by asbestos has engendered concern in potential for a similar risk from high aspect ratio nanoparticles (HARN) such as carbon nanotubes. In the course of studying the potential impact of HARN on the pleura we have utilised the existing hypothesis regarding the role of the parietal pleura in the response to long fibres. This review seeks to synthesise our new data with multi-walled carbon nanotubes (CNT) with that hypothesis for the behaviour of long fibres in the lung and their retention in the parietal pleura leading to the initiation of inflammation and pleural pathology such as mesothelioma. We describe evidence that a fraction of all deposited particles reach the pleura and that a mechanism of particle clearance from the pleura exits, through stomata in the parietal pleura. We suggest that these stomata are the site of retention of long fibres which cannot negotiate them leading to inflammation and pleural pathology including mesothelioma. We cite thoracoscopic data to support the contention, as would be anticipated from the preceding, that the parietal pleura is the site of origin of pleural mesothelioma. This mechanism, if it finds support, has important implications for future research into the mesothelioma hazard from HARN and also for our current view of the origins of asbestos-initiated pleural mesothelioma and the common use of lung parenchymal asbestos fibre burden as a correlate of this tumour, which actually arises in the parietal pleura.
Figures
References
-
- Kane AB, Macdonald JL, Moalli PA. Acute injury and regeneration of mesothelial cells produced by crocidolite asbestos fibers. American Review Of Respiratory Disease. 1986;133:A198.
-
- Boutin C, Dumortier P, Rey F, Viallat JR, De Vuyst P. Black spots concentrate oncogenic asbestos fibers in the parietal pleura. Thoracoscopic and mineralogic study. Am J Respir Crit Care Med. 1996;153:444–449. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
