

Systematic review and meta-analysis of the tolerability and hepatotoxicity of antifungals in empirical and definitive therapy for invasive fungal infection
- PMID: 20308378
- PMCID: PMC2876415
- DOI: 10.1128/AAC.01657-09
Systematic review and meta-analysis of the tolerability and hepatotoxicity of antifungals in empirical and definitive therapy for invasive fungal infection
Abstract
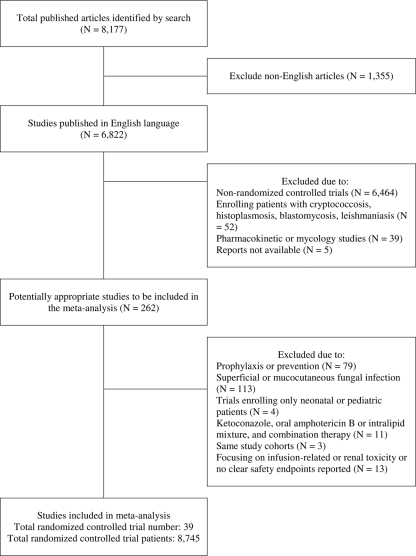
To evaluate the tolerability and liver safety profiles of the systemic antifungal agents commonly used for the treatment of invasive fungal infection, we conducted a systematic review and meta-analysis of randomized controlled trials published before 31 August 2009. Two reviewers independently applied selection criteria, performed quality assessment, and extracted data. We used the beta-binomial model to account for variation across studies and the maximum likelihood method to estimate the pooled risks. We identified 39 studies with more than 8,000 enrolled patients for planned comparisons. The incidence rates of treatment discontinuation due to adverse reactions and liver injury associated with antifungal therapy ranged widely. The pooled risks of treatment discontinuation due to adverse reactions were above 10% for amphotericin B formulations and itraconazole, whereas they were 2.5% to 3.8% for fluconazole, caspofungin, and micafungin. We found that 1.5% of the patients stopped itraconazole treatment due to hepatotoxicity. Furthermore, 19.7% of voriconazole users and 17.4% of itraconazole users had elevated serum liver enzyme levels, although they did not require treatment discontinuation, whereas 2.0% or 9.3% of fluconazole and echinocandin users had elevated serum liver enzyme levels but did not require treatment discontinuation. The results were similar when we stratified the data by empirical or definitive antifungal therapy. Possible explanations for antifungal agent-related hepatotoxicity were confounded by antifungal prescription to patients with a high risk of liver injury, the increased chance of detection of hepatotoxicity due to prolonged treatment, or the pharmacological entity.
Figures
References
-
- Abele-Horn, M., A. Kopp, U. Sternberg, A. Ohly, A. Dauber, W. Russwurm, W. Buchinger, O. Nagengast, and P. Emmerling. 1996. A randomized study comparing fluconazole with amphotericin B/5-flucytosine for the treatment of systemic Candida infections in intensive care patients. Infection 24:426-432. - PubMed
-
- Agresti, A., and B. Coull. 1998. Approximate is better than ‘exact’ for interval estimation of binomial proportions. Am. Stat. 52:119-126.
-
- Anaissie, E. J., R. O. Darouiche, D. Abi-Said, O. Uzun, J. Mera, L. O. Gentry, T. Williams, D. P. Kontoyiannis, C. L. Karl, and G. P. Bodey. 1996. Management of invasive candidal infections: results of a prospective, randomized, multicenter study of fluconazole versus amphotericin B and review of the literature. Clin. Infect. Dis. 23:964-972. - PubMed
-
- Bates, D. W., L. Su, D. T. Yu, G. M. Chertow, D. L. Seger, D. R. Gomes, E. J. Dasbach, and R. Platt. 2001. Mortality and costs of acute renal failure associated with amphotericin B therapy. Clin. Infect. Dis. 32:686-693. - PubMed
-
- Betts, R. F., M. Nucci, D. Talwar, M. Gareca, F. Queiroz-Telles, R. J. Bedimo, R. Herbrecht, G. Ruiz-Palacios, J. A. Young, J. W. Baddley, K. M. Strohmaier, K. A. Tucker, A. F. Taylor, and N. A. Kartsonis. 2009. A multicenter, double-blind trial of a high-dose caspofungin treatment regimen versus a standard caspofungin treatment regimen for adult patients with invasive candidiasis. Clin. Infect. Dis. 48:1676-1684. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
