

Dual-modality breast tomosynthesis
- PMID: 20308457
- PMCID: PMC2843832
- DOI: 10.1148/radiol.09091160
Dual-modality breast tomosynthesis
Abstract
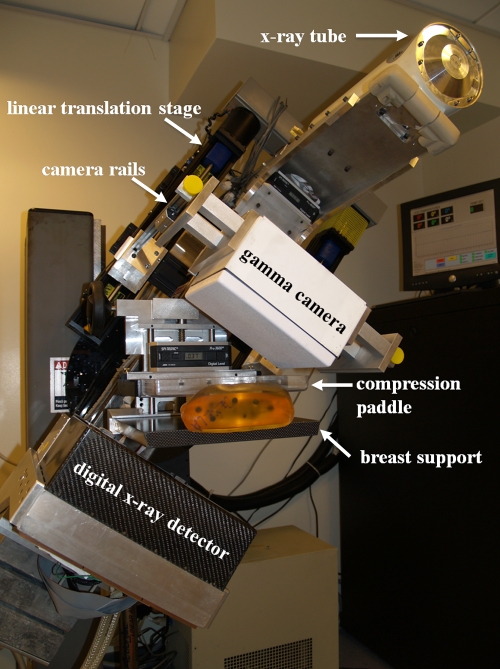
Purpose: To evaluate the clinical performance of a hybrid scanner that uses dual-modality tomosynthesis (DMT) and technetium 99m sestamibi to provide coregistered anatomic and functional breast images in three dimensions.
Materials and methods: A prospective pilot evaluation of the scanner was performed in women scheduled to undergo breast biopsy after institutional review board approval and informed consent were obtained. All subject data were handled in compliance with the rules and regulations concerning the privacy and security of protected health information under HIPAA. The study included 17 women (mean age, 53 years; age range, 44-67 years) and 21 biopsy-sampled lesions. Results of DMT scanning were compared with histopathologic results for the 21 lesions.
Results: Of the 21 lesions, seven were malignant, and 14 were benign. Among the 13 subjects with one lesion each, three had positive biopsy results, and 10 had negative biopsy results. Among the four subjects with two lesions, the biopsy results were as follows: bilateral in one, both negative; bilateral in one, both positive; unilateral in two, one positive and one negative. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of DMT scanning were 86%, 100%, 100%, 93%, and 95%, respectively.
Conclusion: Pilot clinical evaluation of the DMT scanner suggests that it is a feasible and accurate method with which to detect and diagnose breast cancer. Systems such as the DMT scanner that are designed specifically for three-dimensional multimodality breast imaging could make possible some of the advances in tumor detection, localization, and characterization of breast cancer that are now being observed with whole-body three-dimensional hybrid systems, such as positron emission tomography/computed tomography (CT) or single photon emission computed tomography/CT.
RSNA, 2010
Figures
Similar articles
-
Breast-specific gamma imaging as an adjunct imaging modality for the diagnosis of breast cancer.Radiology. 2008 Jun;247(3):651-7. doi: 10.1148/radiol.2473061678. Radiology. 2008. PMID: 18487533
-
Technetium-99m sestamibi scintimammography complements mammography in the detection of breast cancer.Breast J. 2003 Jul-Aug;9(4):288-94. doi: 10.1046/j.1524-4741.2003.09407.x. Breast J. 2003. PMID: 12846862
-
Molecular breast imaging: use of a dual-head dedicated gamma camera to detect small breast tumors.AJR Am J Roentgenol. 2008 Dec;191(6):1805-15. doi: 10.2214/AJR.07.3693. AJR Am J Roentgenol. 2008. PMID: 19020253 Free PMC article.
-
Digital mammography, sestamibi breast scintigraphy, and positron emission tomography breast imaging.Radiol Clin North Am. 2000 Jul;38(4):861-9, x. doi: 10.1016/s0033-8389(05)70206-2. Radiol Clin North Am. 2000. PMID: 10943283 Review.
-
The role of nuclear medicine in breast cancer detection: a focus on Technetium-99 Sestamibi scintimammography.Curr Oncol Rep. 2003 Jan;5(1):58-62. doi: 10.1007/s11912-003-0087-6. Curr Oncol Rep. 2003. PMID: 12493151 Review.
Cited by
-
Dedicated Breast Gamma Camera Imaging and Breast PET: Current Status and Future Directions.PET Clin. 2018 Jul;13(3):363-381. doi: 10.1016/j.cpet.2018.02.008. PET Clin. 2018. PMID: 30100076 Free PMC article. Review.
-
Molecular Breast Imaging using Synthetic Projections from High-Purity Germanium Detectors: A Simulation Study.IEEE Trans Radiat Plasma Med Sci. 2017 Sep;1(5):405-415. doi: 10.1109/TRPMS.2017.2725310. Epub 2017 Jul 11. IEEE Trans Radiat Plasma Med Sci. 2017. PMID: 28989990 Free PMC article.
-
Effects on image quality of a 2D antiscatter grid in x-ray digital breast tomosynthesis: Initial experience using the dual modality (x-ray and molecular) breast tomosynthesis scanner.Med Phys. 2016 Apr;43(4):1720. doi: 10.1118/1.4943632. Med Phys. 2016. PMID: 27036570 Free PMC article.
-
An analysis of the mechanical parameters used for finite element compression of a high-resolution 3D breast phantom.Med Phys. 2011 Oct;38(10):5756-70. doi: 10.1118/1.3637500. Med Phys. 2011. PMID: 21992390 Free PMC article.
-
Comparison of breast specific gamma imaging and molecular breast tomosynthesis in breast cancer detection: Evaluation in phantoms.Med Phys. 2015 Jul;42(7):4250-9. doi: 10.1118/1.4922398. Med Phys. 2015. PMID: 26133623 Free PMC article.
References
-
- Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 part 1):347–360 - PubMed
-
- Carney PA, Miglioretti DL, Yankaskas BC, et al. Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann Intern Med 2003;138(3):168–175 [Published correction appears in Ann Intern Med 2003;138(9):771.] - PubMed
-
- Leconte I, Feger C, Galant C, et al. Mammography and subsequent whole-breast sonography of nonpalpable breast cancers: the importance of radiologic breast density. AJR Am J Roentgenol 2003;180(6):1675–1679 - PubMed
-
- Saunders RS, Jr, Samei E, Lo JY, Baker JA. Can compression be reduced for breast tomosynthesis? Monte Carlo study on mass and microcalcification conspicuity in tomosynthesis. Radiology 2009;251(3):673–682 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
