

Gray zones around diffuse large B cell lymphoma. Conclusions based on the workshop of the XIV meeting of the European Association for Hematopathology and the Society of Hematopathology in Bordeaux, France
- PMID: 20309430
- PMCID: PMC2798939
- DOI: 10.1007/s12308-009-0053-9
Gray zones around diffuse large B cell lymphoma. Conclusions based on the workshop of the XIV meeting of the European Association for Hematopathology and the Society of Hematopathology in Bordeaux, France
Abstract
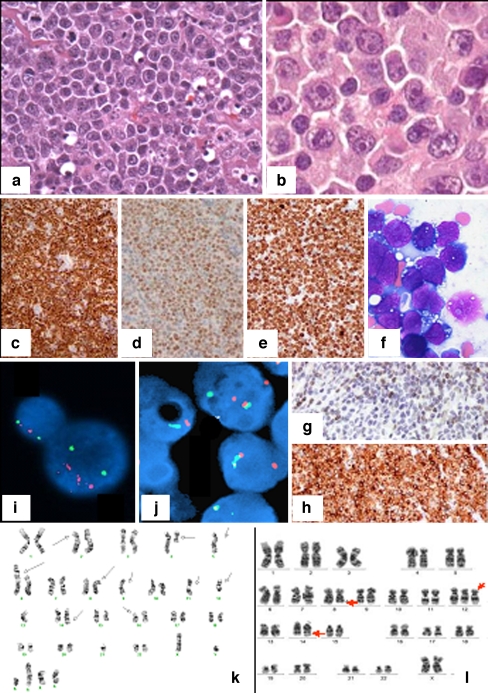
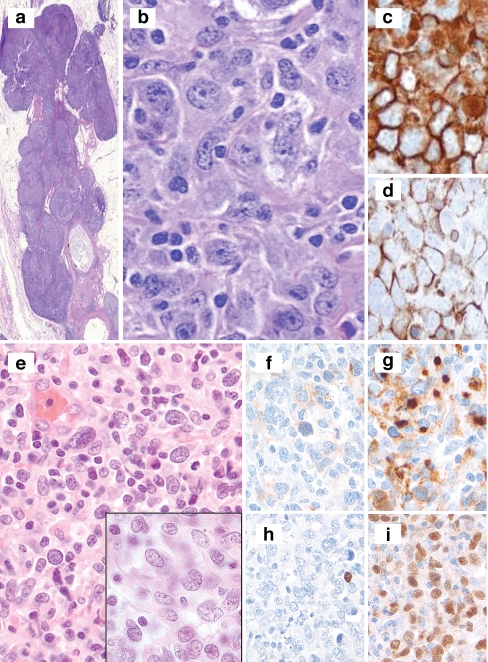
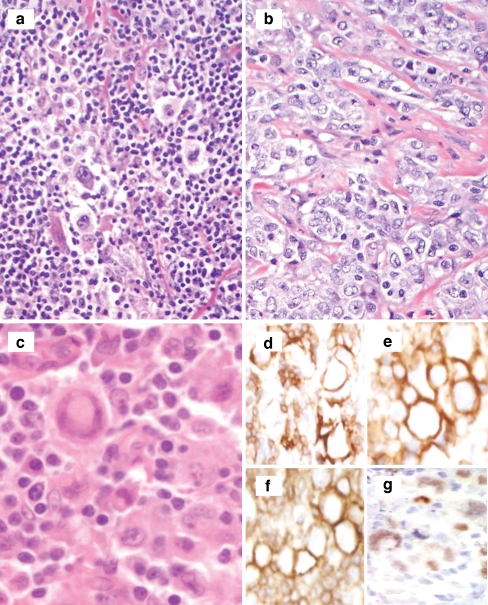
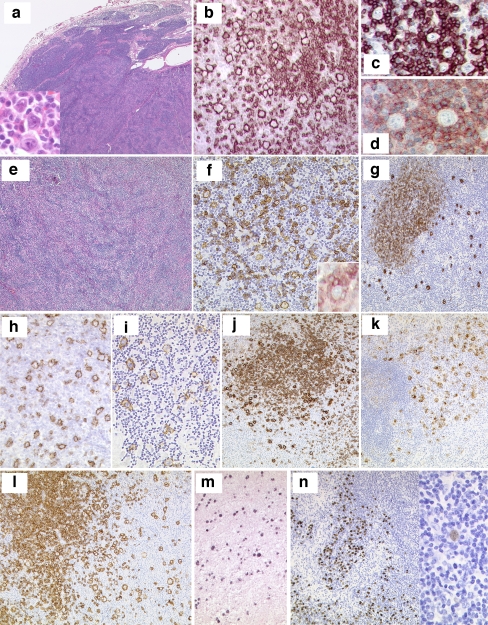
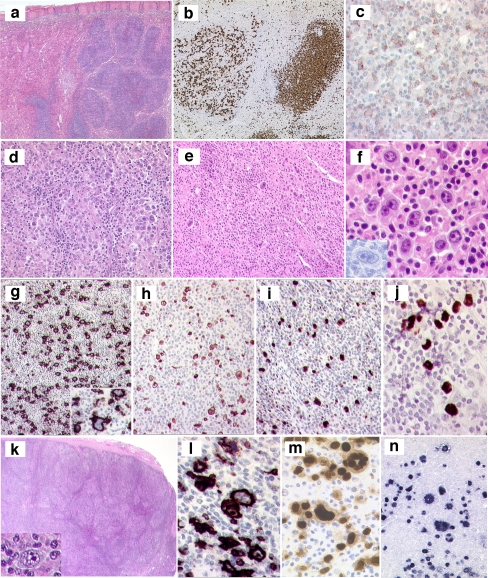
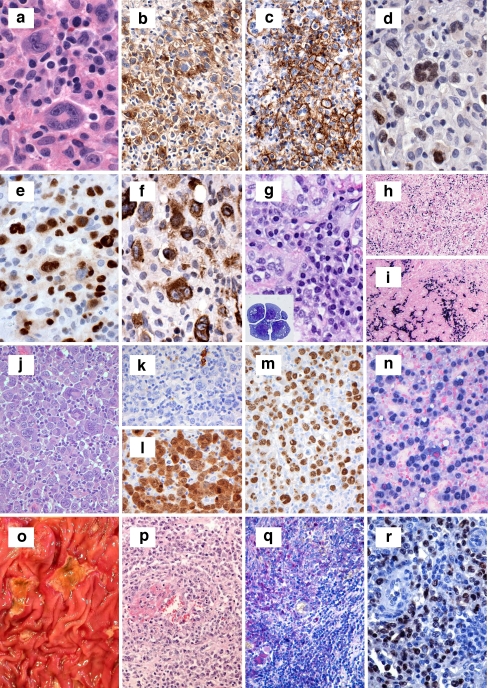
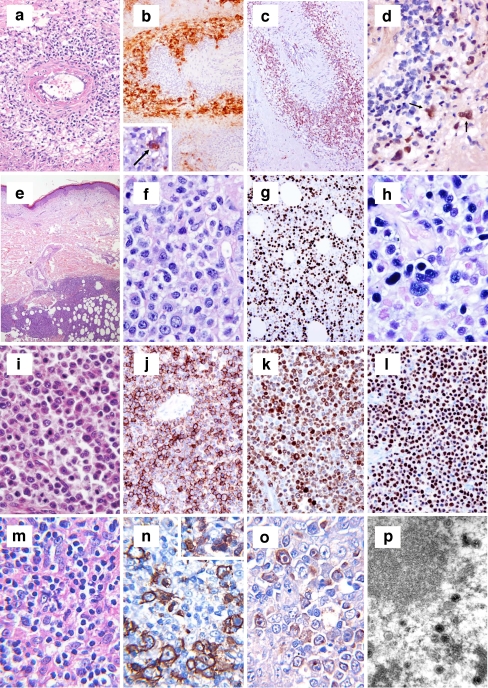
The term "gray-zone" lymphoma has been used to denote a group of lymphomas with overlapping histological, biological, and clinical features between various types of lymphomas. It has been used in the context of Hodgkin lymphomas (HL) and non-Hodgkin lymphomas (NHL), including classical HL (CHL), and primary mediastinal large B cell lymphoma, cases with overlapping features between nodular lymphocyte predominant Hodgkin lymphoma and T-cell/histiocyte-rich large B cell lymphoma, CHL, and Epstein-Barr-virus-positive lymphoproliferative disorders, and peripheral T cell lymphomas simulating CHL. A second group of gray-zone lymphomas includes B cell NHL with intermediate features between diffuse large B cell lymphoma and classical Burkitt lymphoma. In order to review controversial issues in gray-zone lymphomas, a joint Workshop of the European Association for Hematopathology and the Society for Hematopathology was held in Bordeaux, France, in September 2008. The panel members reviewed and discussed 145 submitted cases and reached consensus diagnoses. This Workshop summary is focused on the most controversial aspects of gray-zone lymphomas and describes the panel's proposals regarding diagnostic criteria, terminology, and new prognostic and diagnostic parameters.
Keywords: European Association for Hematopathology; Gray zone lymphoma; Society for Hematopathology; Workshop.
Figures
Similar articles
-
Pitfalls in diagnostic hematopathology -- Part II.Int J Clin Exp Pathol. 2009 Sep 10;3(1):39-46. Int J Clin Exp Pathol. 2009. PMID: 19918327 Free PMC article. Review.
-
Mediastinal large B cell lymphoma and surrounding gray areas: a report of the lymphoma workshop of the 20th meeting of the European Association for Haematopathology.Virchows Arch. 2023 Dec;483(6):733-749. doi: 10.1007/s00428-023-03550-5. Epub 2023 Aug 2. Virchows Arch. 2023. PMID: 37530791 Free PMC article. Review.
-
B-Cell and Classical Hodgkin Lymphomas Associated With Immunodeficiency: 2015 SH/EAHP Workshop Report-Part 2.Am J Clin Pathol. 2017 Feb 1;147(2):153-170. doi: 10.1093/ajcp/aqw216. Am J Clin Pathol. 2017. PMID: 28395108 Free PMC article.
-
GATA3 Immunohistochemical Staining in Hodgkin Lymphoma: Diagnostic Utility in Differentiating Classic Hodgkin Lymphoma From Nodular Lymphocyte Predominant Hodgkin Lymphoma and Other Mimicking Entities.Appl Immunohistochem Mol Morphol. 2019 Mar;27(3):180-184. doi: 10.1097/PAI.0000000000000581. Appl Immunohistochem Mol Morphol. 2019. PMID: 28877074
-
Peripheral T-cell and NK-cell lymphomas and their mimics; taking a step forward - report on the lymphoma workshop of the XVIth meeting of the European Association for Haematopathology and the Society for Hematopathology.Histopathology. 2014 Jan;64(2):171-99. doi: 10.1111/his.12251. Epub 2013 Oct 16. Histopathology. 2014. PMID: 24128129 Free PMC article.
Cited by
-
Clinical, pathological and genetic features of primary mediastinal large B-cell lymphomas and mediastinal gray zone lymphomas in children.Haematologica. 2011 Feb;96(2):262-8. doi: 10.3324/haematol.2010.030809. Epub 2010 Oct 22. Haematologica. 2011. PMID: 20971819 Free PMC article.
-
CD137 is expressed in follicular dendritic cell tumors and in classical Hodgkin and T-cell lymphomas: diagnostic and therapeutic implications.Am J Pathol. 2012 Sep;181(3):795-803. doi: 10.1016/j.ajpath.2012.05.015. Am J Pathol. 2012. PMID: 22901750 Free PMC article.
-
Histopathologic Features and Differential Diagnosis in Challenging Cases of Nodular Lymphocyte Predominant B-cell Lymphoma/Nodular Lymphocyte Predominant Hodgkin Lymphoma.J Clin Transl Pathol. 2024 Jun;4(2):61-69. doi: 10.14218/jctp.2024.00015. J Clin Transl Pathol. 2024. PMID: 39070246 Free PMC article.
-
Mediastinal gray zone lymphoma: clinico-pathological characteristics and outcomes of 99 patients from the Lymphoma Study Association.Haematologica. 2017 Jan;102(1):150-159. doi: 10.3324/haematol.2016.152256. Epub 2016 Oct 6. Haematologica. 2017. PMID: 27758822 Free PMC article.
-
Nodular Lymphocyte Predominant Hodgkin Lymphoma versus T-Cell/Histiocyte-Rich Large B-Cell Lymphoma: A Diagnostic Challenge.Case Rep Pathol. 2014;2014:956217. doi: 10.1155/2014/956217. Epub 2014 Jul 7. Case Rep Pathol. 2014. PMID: 25110597 Free PMC article.
References
-
- Swerdlow SH, et al. WHO classification of tumours of haematopoietic and lymphoid tissues. 4. Lyon: IARC; 2008. - PubMed
-
- Kluin PM, et al. et al. B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma. In: Swerdlow SH, et al.et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. IARC: Lyon; 2008. pp. 265–266.
-
- Jaffe ES, et al. et al. B-cell lymphoma, unclassifiable with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin Lymphoma. In: Swerdlow SH, et al.et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. IARC: Lyon; 2008. pp. 267–268.
-
- Macpherson N, et al. Small noncleaved, non-Burkitt’s (Burkitt-like) lymphoma: cytogenetics predict outcome and reflect clinical presentation. J Clin Oncol. 1999;17(5):1558–1567. - PubMed
-
- Kanungo A, et al. Lymphoid neoplasms associated with concurrent t(14;18) and 8q24/c-MYC translocation generally have a poor prognosis. Mod Pathol. 2006;19(1):25–33. - PubMed
LinkOut - more resources
Full Text Sources
