

Rare lymphoid malignancies of the breast: a report of two cases illustrating potential diagnostic pitfalls
- PMID: 20309431
- PMCID: PMC2798933
- DOI: 10.1007/s12308-009-0043-y
Rare lymphoid malignancies of the breast: a report of two cases illustrating potential diagnostic pitfalls
Abstract
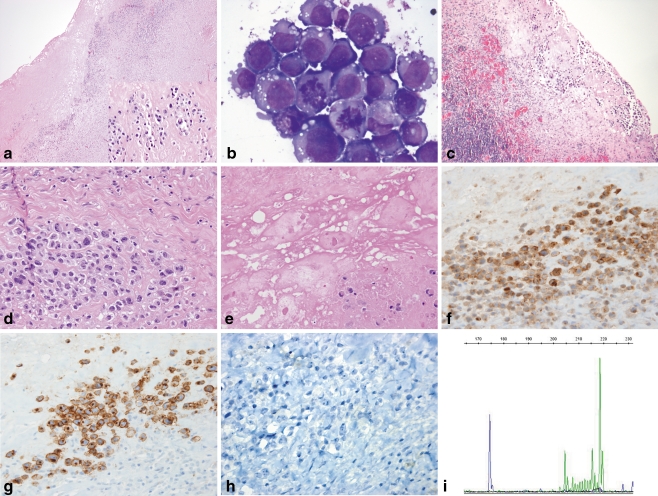
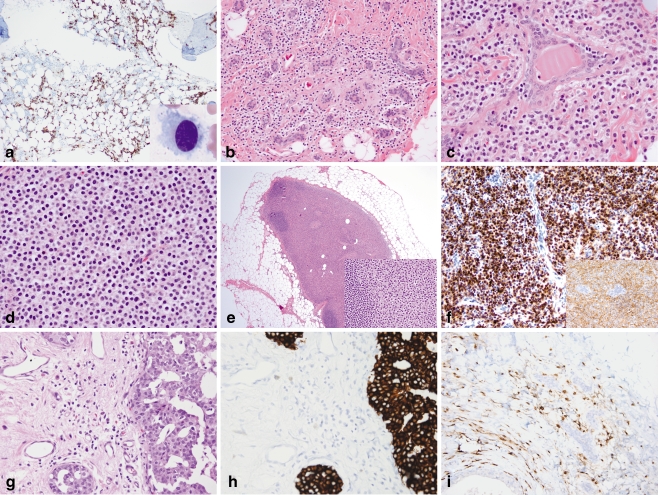
Breast involvement by lymphoma is uncommon and poses challenges in diagnosis. Lymphomas may clinically, radiologically, and morphologically mimic both benign and neoplastic conditions. We describe two cases of lymphoid malignancies predominantly involving the breast, both presenting diagnostic dilemmas. The first case, ALK-negative anaplastic large-cell lymphoma involving a seroma associated with a breast implant, is an emerging clinicopathologic entity. Anaplastic large-cell lymphoma has been identified in association with breast implants and seroma formation relatively recently. The second case, hairy cell leukemia involving the breast and ipsilateral axillary sentinel lymph node, is, to our knowledge, the first reported case of hairy cell leukemia involving the breast at the time of diagnosis. While a localized bone lesion was present at time of diagnosis, bone marrow involvement was relatively mild in comparison to that seen in the breast and lymph node. In the first case, lymphoma occurred in a clinical setting where malignancy was unsuspected, highlighting the importance of careful morphologic evaluation of paucicellular samples, as well as awareness of rare clinicopathologic entities, in avoiding a misdiagnosis of a benign inflammatory infiltrate. In the second case, the lymphoid neoplasm exhibited classic morphologic and immunophenotypic features, but presented at an unusual site of involvement. Knowledge of the patient's concurrent diagnosis of hairy cell leukemia involving the bone marrow and bone helped avoid a misdiagnosis of carcinoma rather than lymphoma.
Keywords: Anaplastic large cell lymphoma; Anaplastic lymphoma kinase; Breast; Breast implant; Hairy cell leukemia; Primary breast lymphoma; Seroma; T-cell neoplasm.
Figures
References
-
- Lamovec J, Wotherspoon A, Jacquemier J. Malignant lymphoma and metastatic tumours. In: Tavassoli F, Devilee P, editors. Tumors of the breast and female genital organs. World Health Organization classification of tumours. Lyon: IARC; 2003. pp. 107–109.
-
- Brogi E, Harris NL. Lymphomas of the breast: pathology and clinical behavior. Semin Oncol. 1999;26:357–364. - PubMed
LinkOut - more resources
Full Text Sources
