

Race versus place of service in mortality among medicare beneficiaries with cancer
- PMID: 20309847
- PMCID: PMC3277834
- DOI: 10.1002/cncr.25097
Race versus place of service in mortality among medicare beneficiaries with cancer
Abstract
Background: Evidence suggests that excess mortality among African-American cancer patients is explained in part by the healthcare setting. The objective of this study was to compare mortality among African-American and Caucasian cancer patients and to evaluate the influence of attendance at a National Cancer Institute (NCI)-designated comprehensive or clinical cancer center.
Methods: The authors conducted a retrospective cohort analysis of Medicare beneficiaries with an incident diagnosis of lung, breast, colorectal, or prostate cancer between 1998 and 2002 who were identified from Surveillance, Epidemiology, and End Results data. Multivariate logistic regression models were used to assess the impact of NCI cancer center attendance and race on all-cause and cancer-specific mortality at 1 year and 3 years after diagnosis.
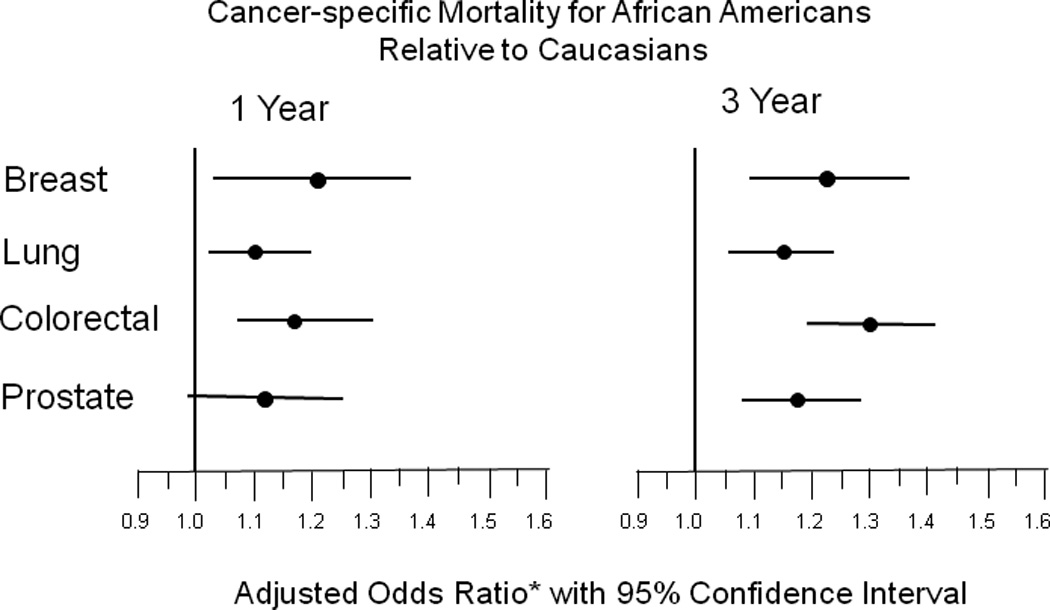
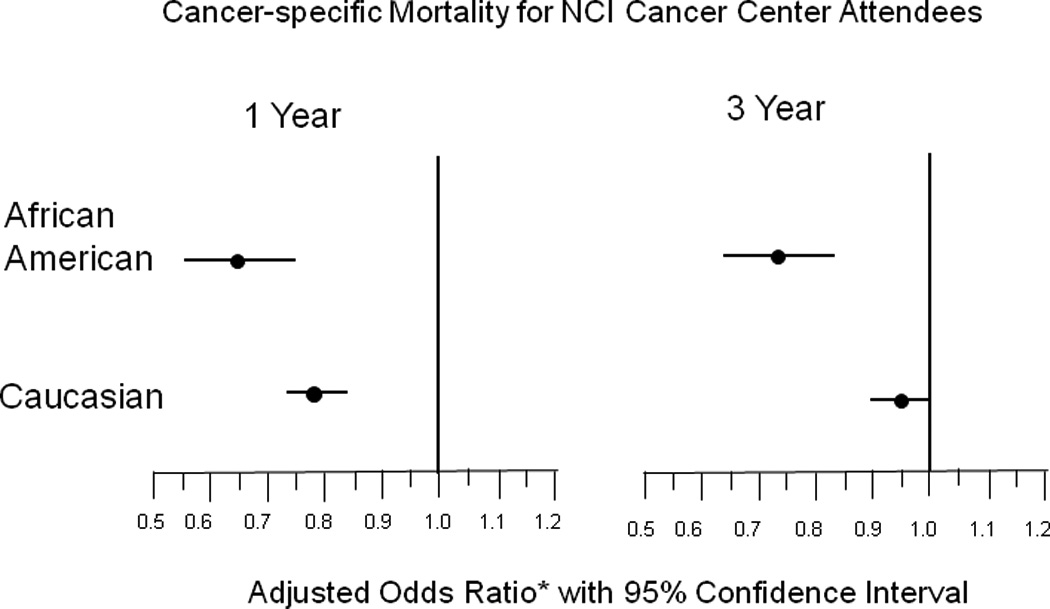
Results: The likelihood of 1-year and 3-year all-cause and cancer-specific mortality was higher for African Americans than for Caucasians in crude and adjusted models (cancer-specific adjusted: Caucasian referent, 1-year odds ratio [OR], 1.13; 95% confidence interval [CI], 1.07-1.19; 3-year OR, 1.23; 95% CI, 1.17-1.30). By cancer site, cancer-specific mortality was higher among African Americans at 1 year for breast and colorectal cancers and for all cancers at 3 years. NCI cancer center attendance was associated with significantly lower odds of mortality for African Americans (1-year OR, 0.63; 95% CI, 0.56-0.76; 3-year OR, 0.71; 95% CI, 0.62-0.81). With Caucasians as the referent group, the excess mortality risk among African Americans no longer was observed for all-cause or cancer-specific mortality risk among patients who attended NCI cancer centers (cancer-specific mortality:1-year OR, 0.95; 95% CI, 0.76-1.19; 3-year OR, 1.00; 95% CI, 0.82-1.21).
Conclusions: African-American Medicare beneficiaries with lung, breast, colorectal, and prostate cancers had higher mortality compared with their Caucasian counterparts; however, there were no significant differences in mortality by race among those who attended NCI cancer centers. The results of this study suggested that place of service may explain some of the cancer mortality excess observed in African Americans.
(c) 2010 American Cancer Society.
Figures
References
-
- Escarce JJ. Racial and ethnic disparities in access to and quality of health care. Robert Wood Johnson Foundation. 2007 Research Synthesis Report No. 12(September). - PubMed
-
- Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S, Begg CB. Survival of blacks and whites after a cancer diagnosis. Jama. 2002;287(16):2106–2113. - PubMed
-
- Hodgson DC, Fuchs CS, Ayanian JZ. Impact of patient and provider characteristics on the treatment and outcomes of colorectal cancer. J Natl Cancer Inst. 2001;93(7):501–515. - PubMed
-
- Baicker K, Chandra A, Skinner JS, Wennberg JE. Who You Are And Where You Live: How Race And Geography Affect The Treatment Of Medicare Beneficiaries. Health Aff (Millwood) 2004 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
