

Cervical cancer prevention: new tools and old barriers
- PMID: 20310056
- PMCID: PMC2876205
- DOI: 10.1002/cncr.25065
Cervical cancer prevention: new tools and old barriers
Abstract
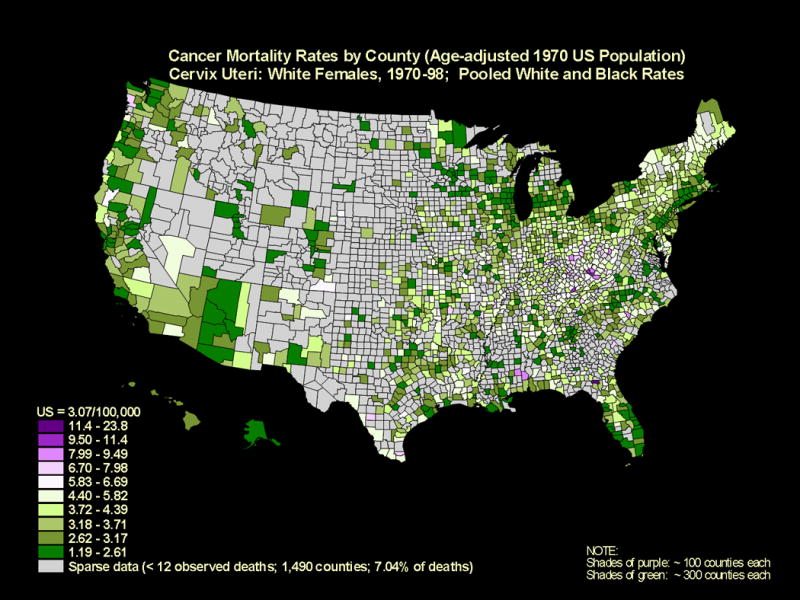
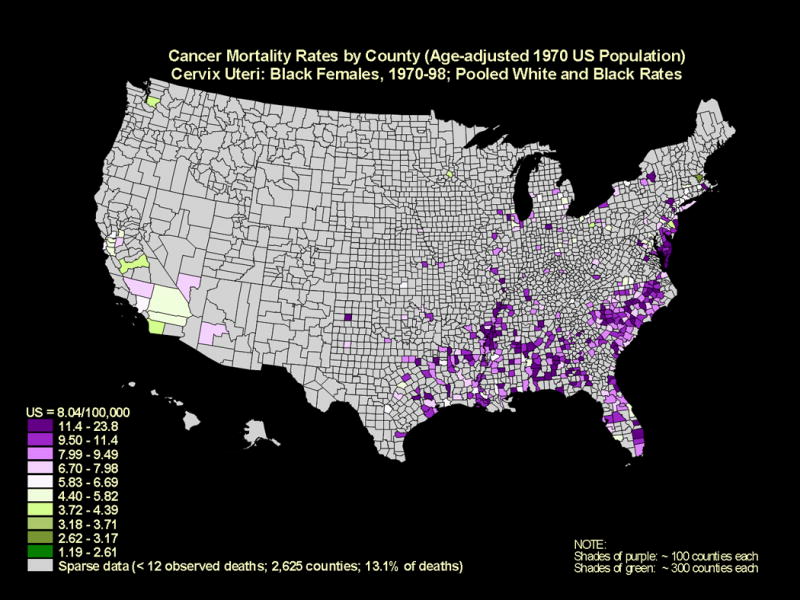
Cervical cancer is the second most common female tumor worldwide, and its incidence is disproportionately high (>80%) in the developing world. In the United States, in which Papanicolaou (Pap) tests have reduced the annual incidence to approximately 11,000 cervical cancers, >60% of cases are reported to occur in medically underserved populations as part of a complex of diseases linked to poverty, race/ethnicity, and/or health disparities. Because carcinogenic human papillomavirus (HPV) infections cause virtually all cervical cancer, 2 new approaches for cervical cancer prevention have emerged: 1) HPV vaccination to prevent infections in younger women (aged < or =18 years) and 2) carcinogenic HPV detection in older women (aged > or =30 years). Together, HPV vaccination and testing, if used in an age-appropriate manner, have the potential to transform cervical cancer prevention, particularly among underserved populations. Nevertheless, significant barriers of access, acceptability, and adoption to any cervical cancer prevention strategy remain. Without understanding and addressing these obstacles, these promising new tools for cervical cancer prevention may be futile. In the current study, the delivery of cervical cancer prevention strategies to these US populations that experience a high cervical cancer burden (African-American women in South Carolina, Alabama, and Mississippi; Haitian immigrant women in Miami; Hispanic women in the US-Mexico Border; Sioux/Native American women in the Northern Plains; white women in the Appalachia; and Vietnamese-American women in Pennsylvania and New Jersey) is reviewed. The goal was to inform future research and outreach efforts to reduce the burden of cervical cancer in underserved populations.
(c) 2010 American Cancer Society.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Schiffman M, Castle PE, Jeronimo J, Rodriguez AC, Wacholder S. Human papillomavirus and cervical cancer. Lancet. 2007;370:890–907. - PubMed
-
-
Centers for Disease Control and Prevention: Cervical Cancer. 2009.
-
-
-
Surveillance, Epidemiology and End Results (SEER) Program. 2009.
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
