

Heterogeneity in malaria exposure and vaccine response: implications for the interpretation of vaccine efficacy trials
- PMID: 20331863
- PMCID: PMC2851701
- DOI: 10.1186/1475-2875-9-82
Heterogeneity in malaria exposure and vaccine response: implications for the interpretation of vaccine efficacy trials
Abstract
Background: Phase III trials of the malaria vaccine, RTS, S, are now underway across multiple sites of varying transmission intensity in Africa. Heterogeneity in exposure, vaccine response and waning of efficacy may bias estimates of vaccine efficacy.
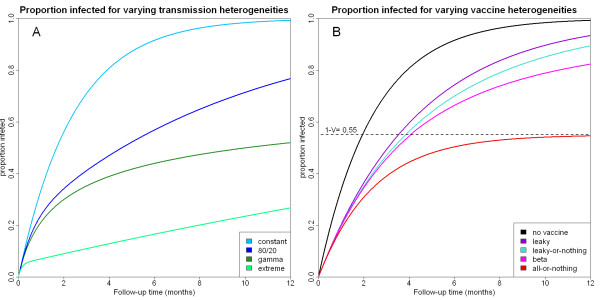
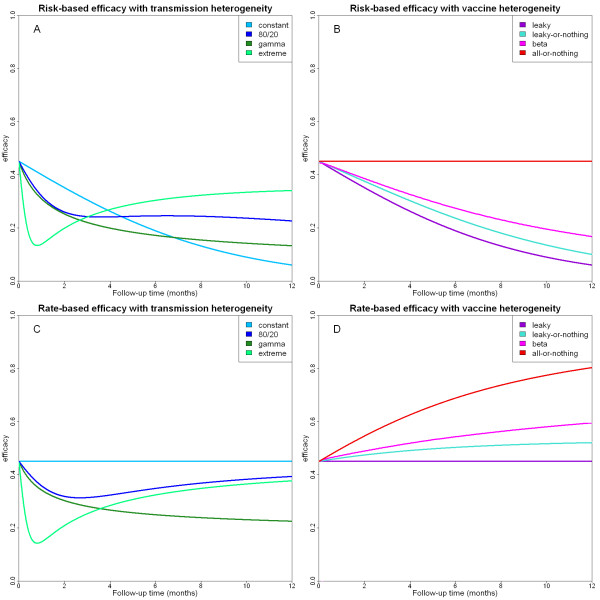
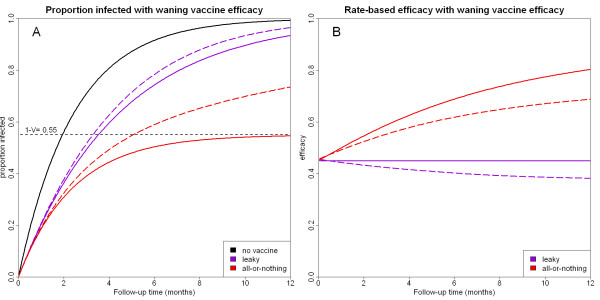
Methods: Theoretical arguments are used to identify the expected effects of a) heterogeneity in exposure to infectious bites; b) heterogeneity in individual's response to the vaccine; and c) waning efficacy on measures of vaccine efficacy from clinical trials for an infection-blocking vaccine.
Results: Heterogeneity in exposure and vaccine response leads to a smaller proportion of trial participants becoming infected than one would expect in a homogeneous setting. This causes estimates of vaccine efficacy from clinical trials to be underestimated if transmission heterogeneity is ignored, and overestimated if heterogeneity in vaccine response is ignored. Waning of vaccine efficacy can bias estimates of vaccine efficacy in both directions.
Conclusions: Failure to account for heterogeneities in exposure and response, and waning of efficacy in clinical trials can lead to biased estimates of malaria vaccine efficacy. Appropriate methods to reduce these biases need to be used to ensure accurate interpretation and comparability between trial sites of results from the upcoming Phase III clinical trials of RTS, S.
Figures
References
-
- Ceesay SJ, Casals-Pascual C, Erskine J, Anya SE, Duah NO, Fulford AJ, Sesay SS, Abubakar I, Dunyo S, Sey O, Palmer A, Fofana M, Corrah T, Bojang KA, Whittle HC, Greenwood BM, Conway DJ. Changes in malaria indices between 1999 and 2007 in The Gambia: a retrospective analysis. The Lancet. 2008;372:1545–1554. doi: 10.1016/S0140-6736(08)61654-2. - DOI - PMC - PubMed
-
- Alonso PL, Sacarlal J, Aponte JJ, Leach A, Macete E, Milman J, Mandomando I, Spiessens B, Guinovart C, Espasa M, Bassat Q, Aide P, Ofori-Anyinam O, Navia MM, Corachan S, Ceuppens M, Dubois M-C, Demoitié M-A, Dubovsky F, Menéndez C, Tornieporth N, Ballou WR, Thompson R, Cohen J. Efficacy of the RTS, S/AS02A vaccine against Plasmodium falciparum infection and disease in young African children: randomised controlled trial. Lancet. 2004;364:1411–1420. doi: 10.1016/S0140-6736(04)17223-1. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
