

Classification and management of refractory coeliac disease
- PMID: 20332526
- PMCID: PMC2861306
- DOI: 10.1136/gut.2009.195131
Classification and management of refractory coeliac disease
Abstract
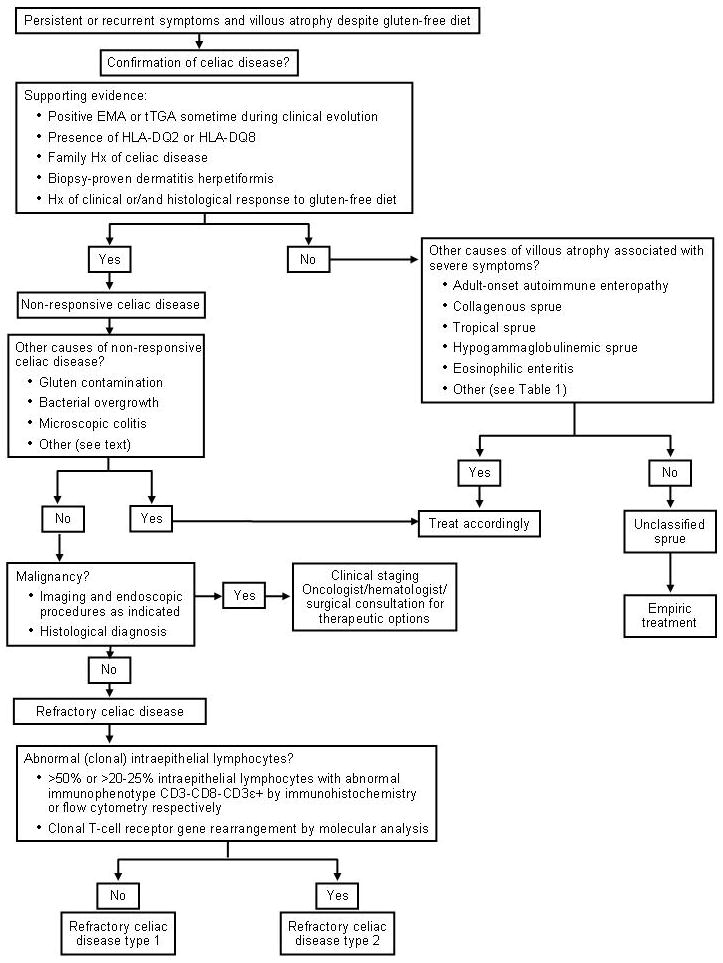
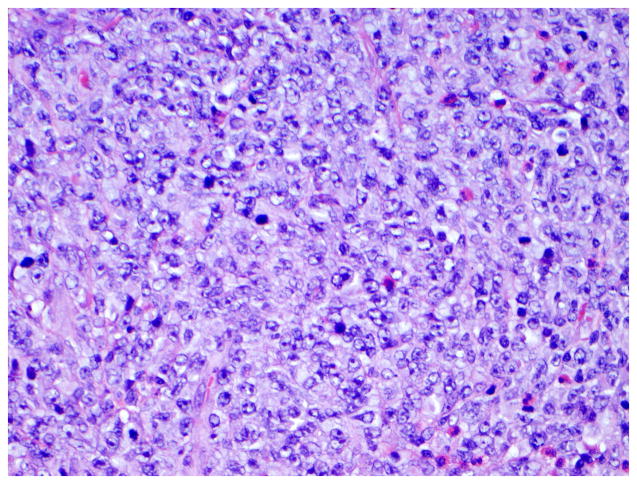
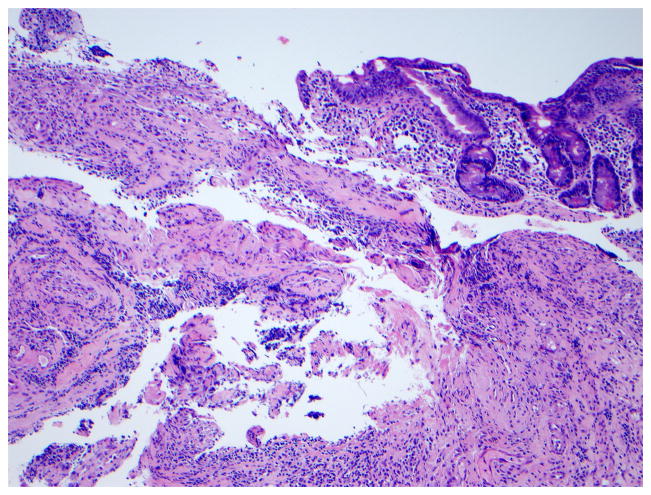
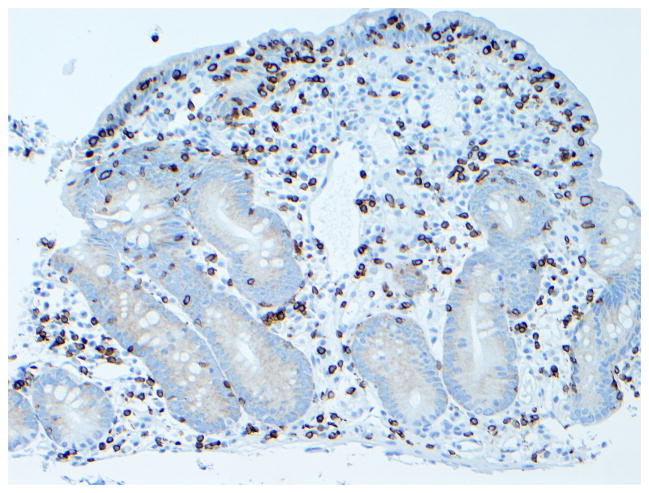
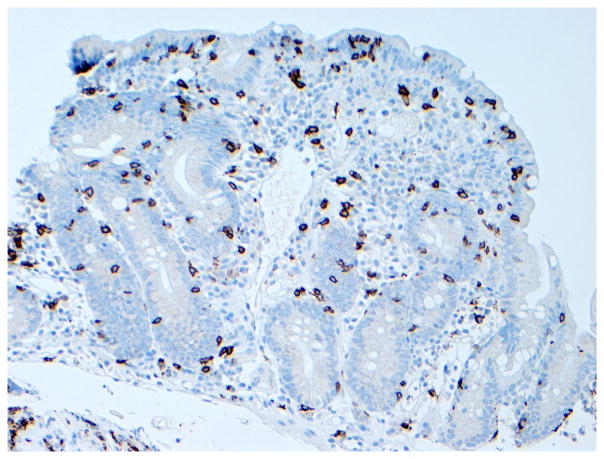
Refractory coeliac disease (RCD) is defined by persistent or recurrent malabsorptive symptoms and villous atrophy despite strict adherence to a gluten-free diet (GFD) for at least 6-12 months in the absence of other causes of non-responsive treated coeliac disease and overt malignancy. Symptoms are often severe and require additional therapeutic intervention besides a GFD. RCD can be classified as type 1 (normal intraepithelial lymphocyte phenotype), or type 2 (defined by the presence of abnormal (clonal) intraepithelial lymphocyte phenotype). Patients with RCD may never have responded to a GFD or may have relapsed despite adherence and initial response to the GFD. RCD type 1 usually improves after treatment with a combination of aggressive nutritional support, adherence to a GFD, and alternative pharmacological therapies. By contrast, clinical response to alternative therapies in RCD type 2 is less certain and the prognosis is poor. Severe complications such as ulcerative jejunitis and enteropathy-associated T cell lymphoma may occur in a subgroup of patients with RCD. The aims of this article are to (1) review recent advances in the diagnosis and management of patients with RCD, and (2) describe current and novel methods for classification of patients with RCD into categories that are useful to predict outcome and direct treatment.
Conflict of interest statement
Figures

References
-
- Di Sabatino A, Corazza GR. Coeliac disease. Lancet. 2009;373:1480–93. - PubMed
-
- Catassi C. The world map of celiac disease. Acta Gastroenterol Latinoam. 2005;35:37–55. - PubMed
-
- Lohi S, Mustalahti K, Kaukinen K, Laurila K, Collin P, Rissanen H, Lohi O, Bravi E, Gasparin M, Reunanen A, Maki M. Increasing prevalence of coeliac disease over time. Aliment Pharmacol Ther. 2007;26:1217–25. - PubMed
-
- Green PH, Cellier C. Celiac disease. N Engl J Med. 2007;357:1731–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical