

Algorithms to predict cerebral malaria in murine models using the SHIRPA protocol
- PMID: 20334682
- PMCID: PMC2850361
- DOI: 10.1186/1475-2875-9-85
Algorithms to predict cerebral malaria in murine models using the SHIRPA protocol
Abstract
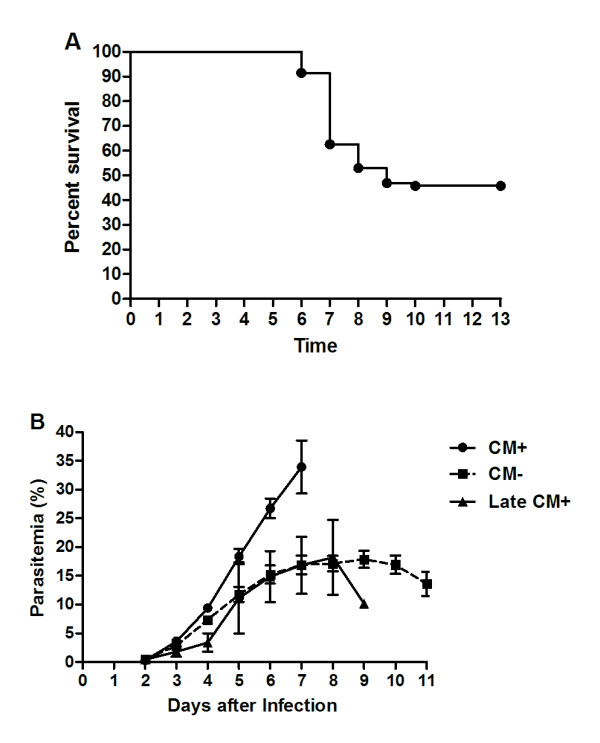
Background: Plasmodium berghei ANKA infection in C57Bl/6 mice induces cerebral malaria (CM), which reproduces, to a large extent, the pathological features of human CM. However, experimental CM incidence is variable (50-100%) and the period of incidence may present a range as wide as 6-12 days post-infection. The poor predictability of which and when infected mice will develop CM can make it difficult to determine the causal relationship of early pathological changes and outcome. With the purpose of contributing to solving these problems, algorithms for CM prediction were built.
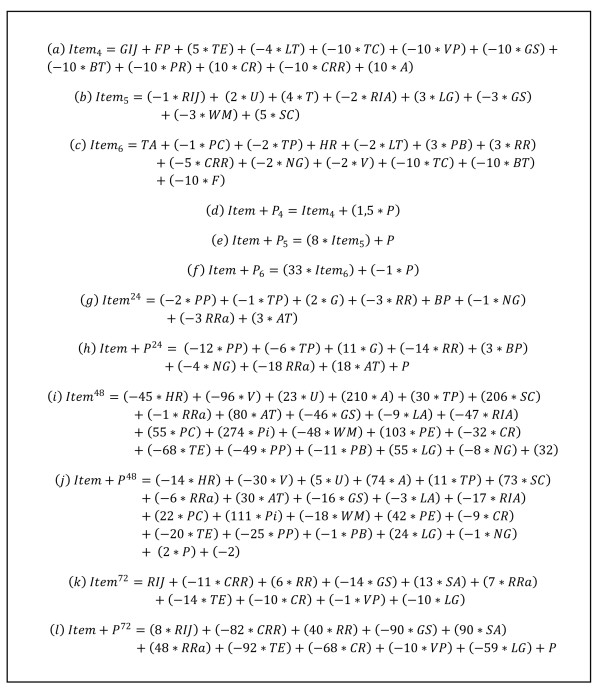
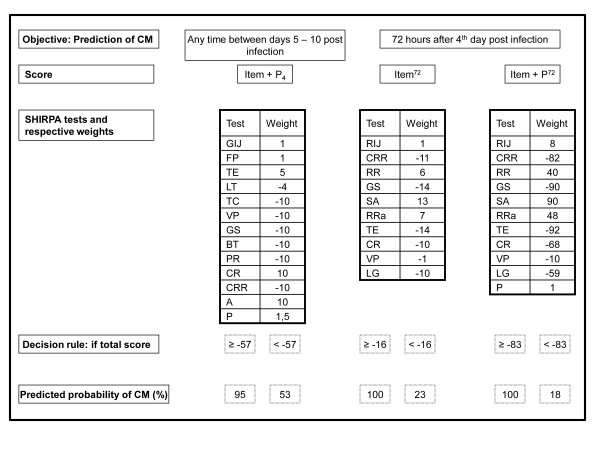
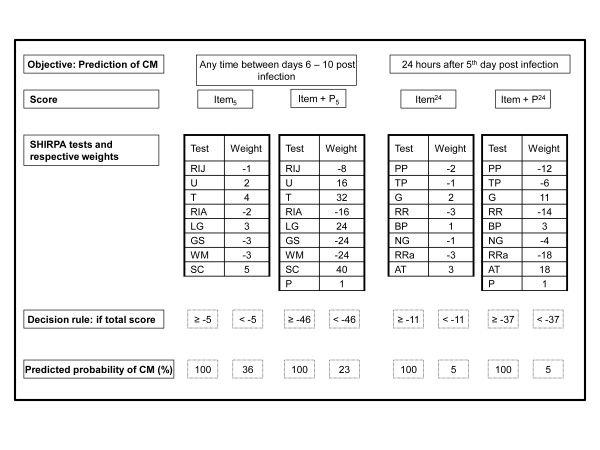
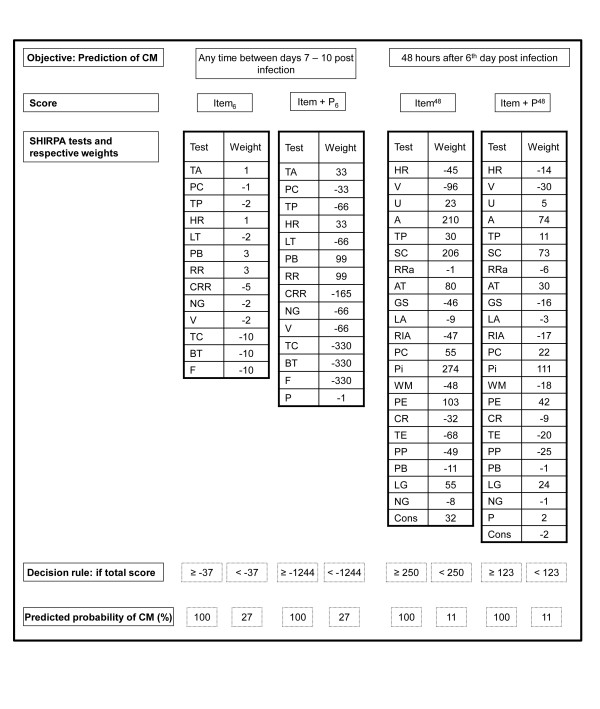
Methods: Seventy-eight P. berghei-infected mice were daily evaluated using the primary SHIRPA protocol. Mice were classified as CM+ or CM- according to development of neurological signs on days 6-12 post-infection. Logistic regression was used to build predictive models for CM based on the results of SHIRPA tests and parasitaemia.
Results: The overall CM incidence was 54% occurring on days 6-10. Some algorithms had a very good performance in predicting CM, with the area under the receiver operator characteristic ((au)ROC) curve > or = 80% and positive predictive values (PV+) > or = 95, and correctly predicted time of death due to CM between 24 and 72 hours before development of the neurological syndrome ((au)ROC = 77-93%; PV+ = 100% using high cut off values). Inclusion of parasitaemia data slightly improved algorithm performance.
Conclusion: These algorithms work with data from a simple, inexpensive, reproducible and fast protocol. Most importantly, they can predict CM development very early, estimate time of death, and might be a valuable tool for research using CM murine models.
Figures
References
-
- Alves FP, Durlacher RR, Menezes MJ, Krieger H, Silva LH, Camargo EP. High prevalence of asymptomatic Plasmodium vivax and Plasmodium falciparum infections in native Amazonian populations. Am J Trop Med Hyg. 2002;66:641–648. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
