

Conservative management of well-differentiated thyroid cancer
- PMID: 20334743
- PMCID: PMC2845956
Conservative management of well-differentiated thyroid cancer
Abstract
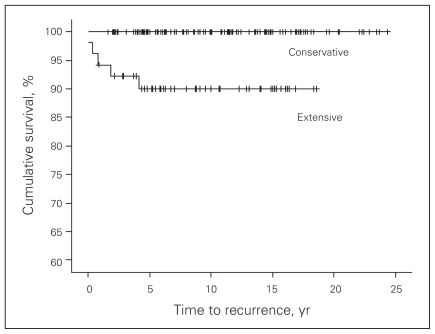
Background: Controversy exists over the optimal surgical treatment of well-differentiated thyroid cancer. Conservative surgical management reduces the risk of complications and maintains an overall survival rate equivalent to the more extensive approach.
Methods: We conducted a retrospective review of all patients with well-differentiated thyroid cancer greater than 1 cm (180 patients) who underwent surgery between 1982 and 2002 by a single general surgeon at our institution. The prevailing philosophy was to be as conservative as possible, and the predominant resection was lobectomy and isthmusectomy on the affected side.
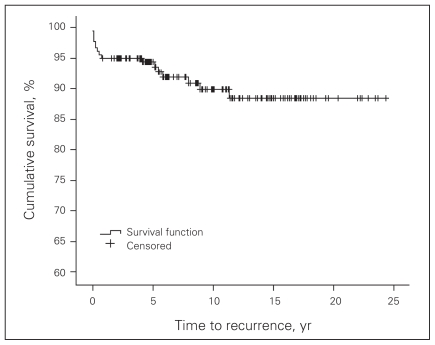
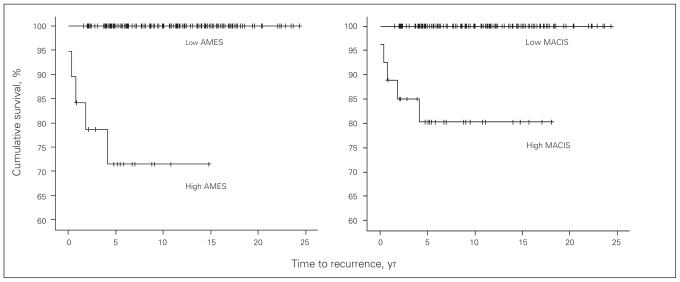
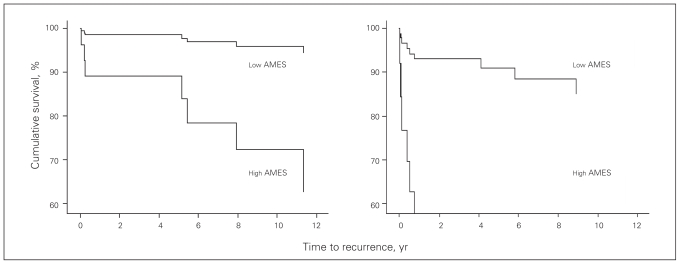
Results: In total, 90% of patients were in a definable low-risk group: 75% had conservative surgery with 4 recurrences and no mortality, 25% had extensive surgery with 3 recurrences and no mortality. The other 10% were in a definable high-risk group: 90% had extensive surgery with 9 recurrences and 4 deaths. Overall, there were 22 sites of recurrence in 16 patients. There was no recurrence in the residual thyroid tissue, with a median follow-up of 10 years. Three recurrences occurred in the resected thyroid bed; each of these patients had undergone extensive surgery. Twelve recurrences were in lymph nodes; 67% of these patients had extensive surgery. All except 1 of 7 distant metastases occurred in the high-risk group, despite the patient having undergone extensive local surgery. Recurrence did not affect survival in the low-risk group. The extensive surgery group had a 3.4% incidence of recurrent laryngeal nerve injury and a 1.1% incidence of permanent hypocalcemia, with none in the conservative surgery group.
Conclusion: Conservative surgery for low-risk patients with well-differentiated thyroid cancer appears to be sufficient and avoids complications without significantly increased risk for local, regional or distant recurrence.
Contexte: Le traitement chirurgical optimal d’un cancer de la thyroïde bien différencié soulève la controverse. Le traitement chirurgical conservateur réduit le risque de complications et maintient un taux de survie global équivalant à celui de l’approche plus étendue.
Méthodes: Nous avons effectué une étude rétrospective portant sur tous les patients atteints d’un cancer de la thyroïde bien différencié de plus de 1 cm (180 patients) qui ont subi, entre 1982 et 2002, une intervention chirurgicale pratiquée par le même chirurgien généraliste à notre établissement. La philosophie dominante consistait à être aussi conservateur que possible et la lobectomie et l’isthmectomie du côté atteint constituaient la principale résection.
Résultats: Au total, 90 % des patients se trouvaient dans un groupe à faible risque définissable : 75 % ont subi une intervention chirurgicale conservatrice à la suite de laquelle il y a eu quatre récurrences et aucune mortalité, 25 % ont subi une intervention chirurgicale étendue à la suite de laquelle il y a eu trois récurrences et aucune mortalité. L’autre tranche de 10 % constituait un groupe à risque élevé définissable : 90 % des patients de ce groupe ont subi une intervention chirurgicale étendue à la suite de laquelle il y a eu 9 récurrences et 4 décès. Dans l’ensemble, le cancer est réapparu à 22 endroits chez 16 patients. Il n’y a pas eu de récurrence dans le reste de tissu thyroïdien à un suivi médian de 10 ans. Il y a eu 3 récurrences dans le lit thyroïdien réséqué : chacun des patients en cause avait subi une intervention chirurgicale étendue. Les 7 métastases éloignées sauf une ont fait leur apparition chez les patients du groupe à risque élevé même si le patient avait subi une intervention chirurgicale locale étendue. La récurrence n’a pas eu d’effet sur la survie des patients du groupe à faible risque. Les patients du groupe ayant subi une intervention chirurgicale étendue présentaient une incidence de 3,4 % de répétition du traumatisme du nerf laryngien et une incidence de 1,1 % d’hypocalcémie permanente, ce qui ne s’est pas produit chez les patients ayant subi une intervention chirurgicale conservatrice.
Conclusion: L’intervention chirurgicale conservatrice chez les patients à faible risque qui ont un cancer de la thyroïde bien différencié semble suffire et évite les complications sans accroître considérablement le risque de récurrence locale, régionale ou éloignée.
Figures
References
-
- Jatzko GR, Lisborg PH, Muller MG, et al. Recurrent nerve palsy after thyroid operations — principal nerve identification and a literature review. Surgery. 1994;115:139–44. - PubMed
-
- Moulton-Barrett R, Crumley R, Jalilie S, et al. Complications of thyroid surgery. Int Surg. 1997;82:63–6. - PubMed
-
- Filho JG, Kowalski LP. Postoperative complications of thyroidectomy for differentiated thyroid carcinoma. Am J Otolaryngol. 2004;25:225–30. - PubMed
-
- Mazzaferri EL. An overview of the management of papillary and follicular thyroid carcinoma. Thyroid. 1999;9:421–7. - PubMed
-
- Shaha AR, Shah JP, Loree TR. Low-risk differentiated thyroid cancer: the need for selective treatment. Ann Surg Oncol. 1997;4:328–33. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical