

Evaluation of left atrial lesions after initial and repeat atrial fibrillation ablation: lessons learned from delayed-enhancement MRI in repeat ablation procedures
- PMID: 20335558
- PMCID: PMC3128796
- DOI: 10.1161/CIRCEP.109.868356
Evaluation of left atrial lesions after initial and repeat atrial fibrillation ablation: lessons learned from delayed-enhancement MRI in repeat ablation procedures
Abstract
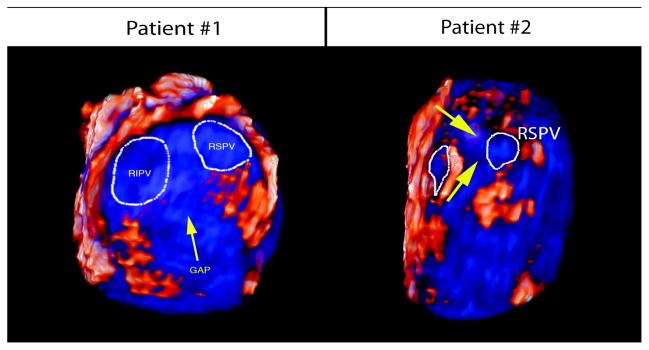
Background: We evaluated scar lesions after initial and repeat catheter ablation of atrial fibrillation (AF) and correlated these regions to low-voltage tissue on repeat electroanatomic mapping. We also identified gaps in lesion sets that could be targeted and closed during repeat procedures.
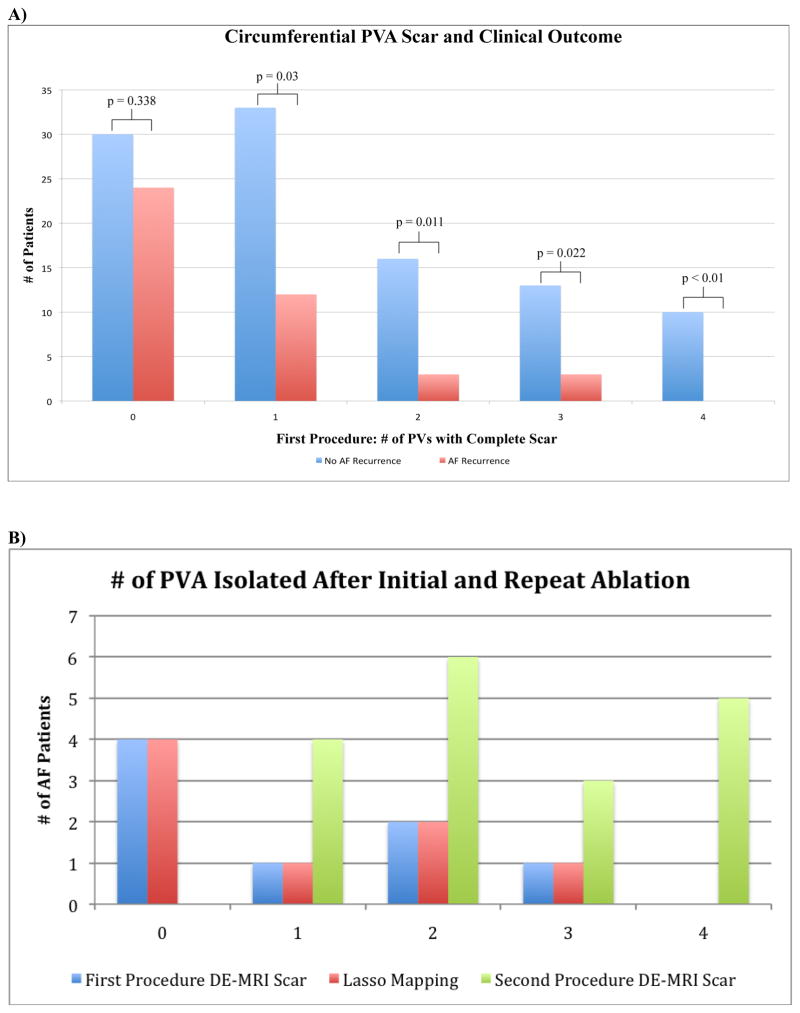
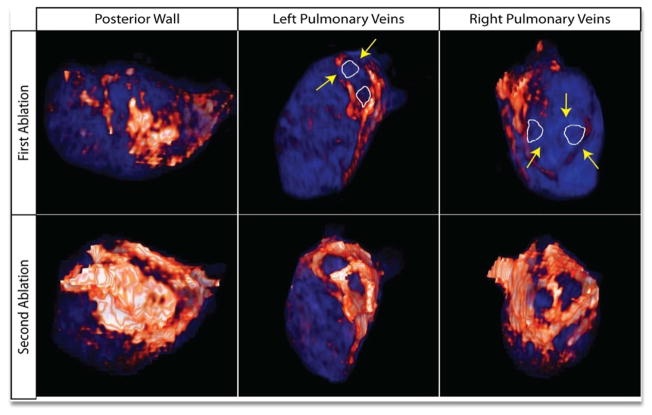
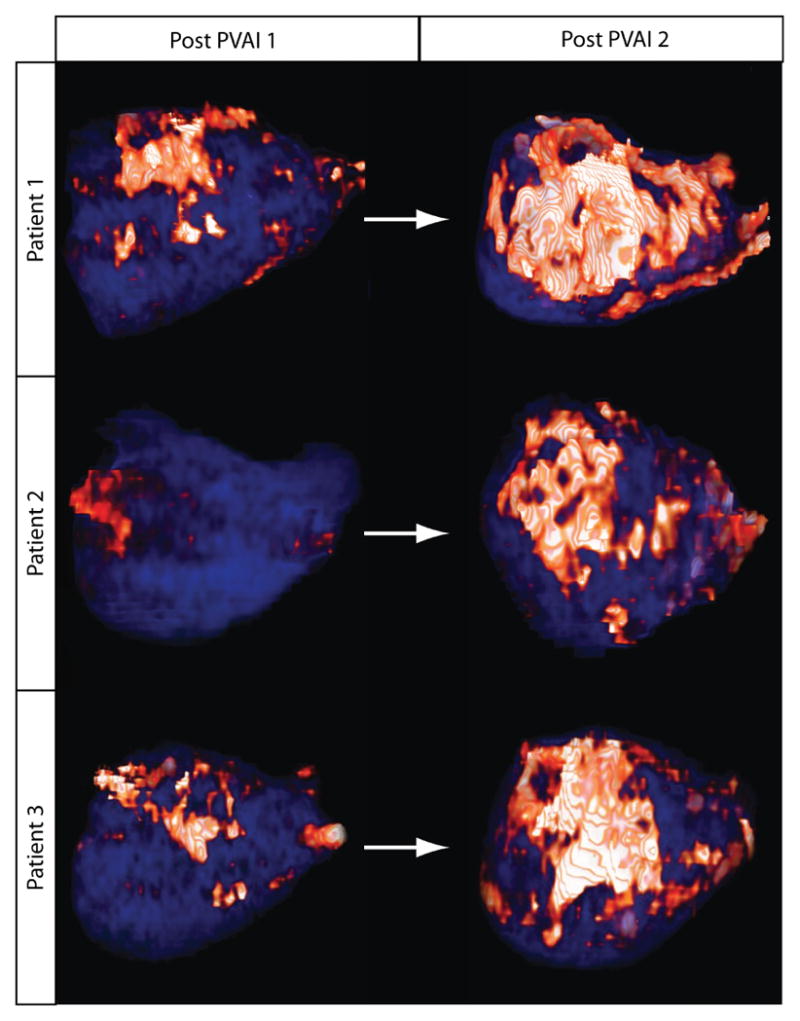
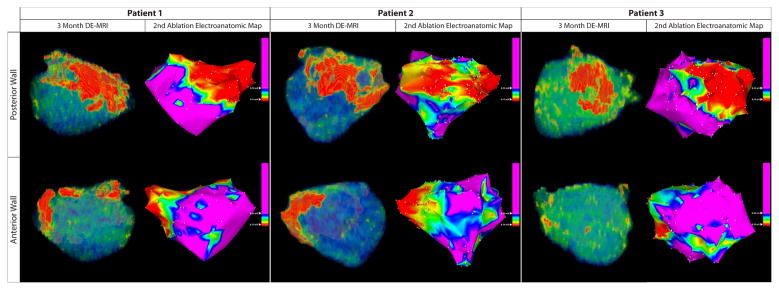
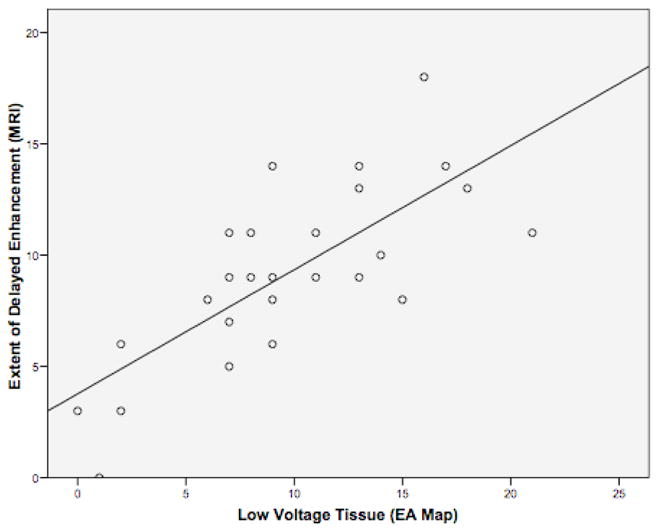
Methods and results: One hundred forty-four patients underwent AF ablation and received a delayed-enhancement MRI at 3 months after ablation. The number of pulmonary veins (PV) with circumferential lesions were assessed and correlated with procedural outcome. Eighteen patients with AF recurrence underwent repeat ablation. MRI scar regions were compared with electroanatomic maps during the repeat procedure. Regions of incomplete scar around the PVs were then identified and targeted during repeat ablation to ensure complete circumferential lesions. After the initial procedure, complete circumferential scarring of all 4 PV antrum (PVA) was achieved in only 7% of patients, with the majority of patients (69%) having <2 completely scarred PVA. After the first procedure, the number of PVs with complete circumferential scarring and total left atrial wall (LA) scar burden was associated with better clinical outcome. Patients with successful AF termination had higher average total left atrial wall scar of 16.4%+/-9.8 (P=0.004) and percent PVA scar of 66.2+/-25.4 (P=0.01) compared with patients with AF recurrence who had an average total LA wall scar 11.3%+/-8.1 and PVA percent scar 50.0+/-24.7. In patients who underwent repeat ablation, the PVA scar percentage was 56.1%+/-21.4 after the first procedure compared with 77.2%+/-19.5 after the second procedure. The average total LA scar after the first ablation was 11.0%+/-4.1, whereas the average total LA scar after second ablation was 21.2%+/-7.4. All patients had an increased number of completely scarred pulmonary vein antra after the second procedure. MRI scar after the first procedure and low-voltage regions on electroanatomic mapping obtained during repeat ablation demonstrated a positive quantitative correlation of R(2)=0.57.
Conclusions: Complete circumferential PV scarring difficult to achieve but is associated with better clinical outcome. Delayed-enhancement MRI can accurately define scar lesions after AF ablation and can be used to target breaks in lesion sets during repeat ablation.
Conflict of interest statement
Figures
References
-
- Marrouche NF, Guenther J, Segerson NM, Daccarett M, Rittger H, Marschang H, Schibgilla V, Schmidt M, Ritscher G, Noelker G, Brachmann J. Randomized comparison between open irrigation technology and intracardiac-echo-guided energy delivery for pulmonary vein antrum isolation: procedural parameters, outcomes, and the effect on esophageal injury. J Cardiovasc Electrophysiol. 2007;18:583–588. - PubMed
-
- Pappone C, Oreto G, Rosanio S, Vicedomini G, Tocchi M, Gugliotta F, Salvati A, Dicandia C, Calabro MP, Mazzone P, Ficarra E, Di Gioia C, Gulletta S, Nardi S, Santinelli V, Benussi S, Alfieri O. Atrial electroanatomic remodeling after circumferential radiofrequency pulmonary vein ablation: efficacy of an anatomic approach in a large cohort of patients with atrial fibrillation. Circulation. 2001;104:2539–2544. - PubMed
-
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. New England Journal of Medicine. 1998;339:656–666. - PubMed
-
- Verma A, Kilicaslan F, Pisano E, Marrouche NF, Fanelli R, Brachmann J, Geunther J, Potenza D, Martin DO, Cummings J, Burkhardt JD, Saliba W, Schweikert RA, Natale A. Response of atrial fibrillation to pulmonary vein antrum isolation is directly related to resumption and delay of pulmonary vein conduction. Circulation. 2005;112:627–635. - PubMed
-
- McGann CJ, Kholmovski EG, Oakes RS, Blauer JJ, Daccarett M, Segerson N, Airey KJ, Akoum N, Fish E, Badger TJ, DiBella EV, Parker D, MacLeod RS, Marrouche NF. New magnetic resonance imaging-based method for defining the extent of left atrial wall injury after the ablation of atrial fibrillation. J Am Coll Cardiol. 2008;52:1263–1271. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
