

Effectiveness of medications used to attenuate antipsychotic-related weight gain and metabolic abnormalities: a systematic review and meta-analysis
- PMID: 20336059
- PMCID: PMC3055458
- DOI: 10.1038/npp.2010.21
Effectiveness of medications used to attenuate antipsychotic-related weight gain and metabolic abnormalities: a systematic review and meta-analysis
Abstract
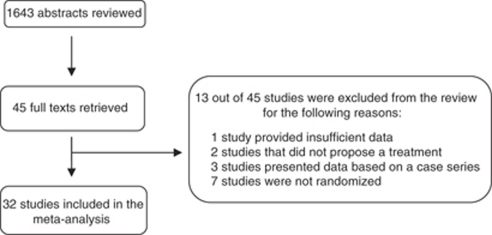
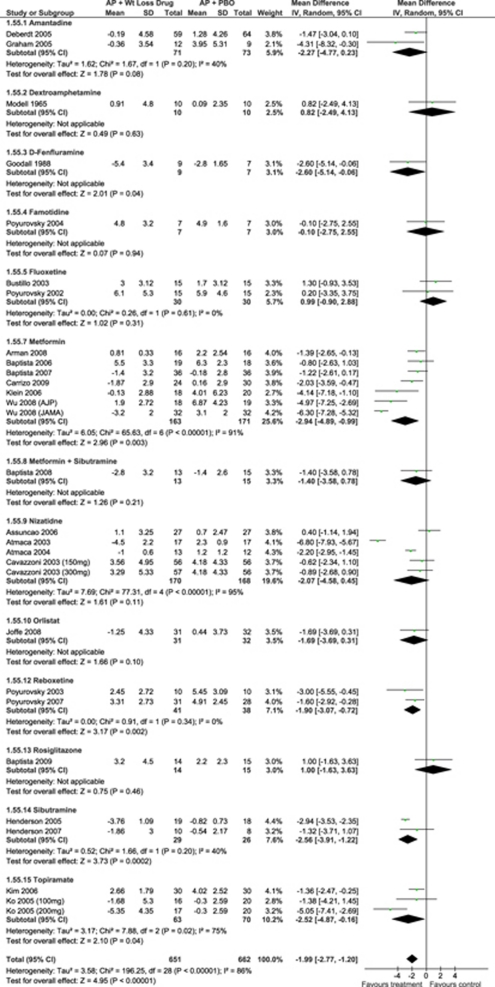
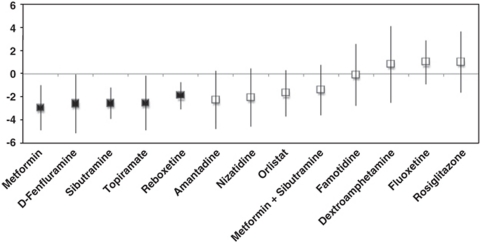
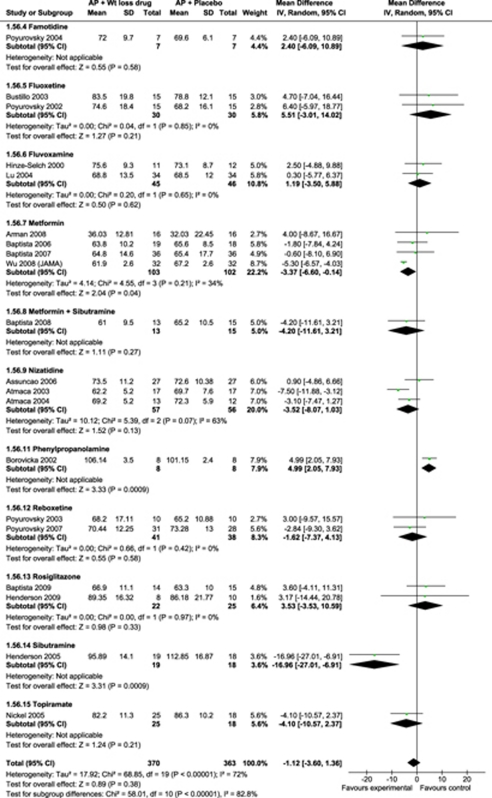
Antipsychotic-related weight gain and metabolic effects are a critical outcome for patients requiring these medications. A literature search using MEDLINE, Web of Science, PsycNET, and EMBASE for randomized, open and double-blind, placebo-controlled trials of medications targeting antipsychotic-induced weight gain was performed. Primary outcome measures were change and endpoint values in body weight and body mass index (BMI). Secondary outcomes included >or=7% weight gain, all-cause discontinuation, change in waist circumference, glucose and lipid metabolism parameters, and psychiatric symptoms. Sensitivity analyses were conducted to explain heterogeneity of the results. Across 32 studies including 1482 subjects, 15 different medications were tested: amantadine, dextroamphetamine, d-fenfluramine, famotidine, fluoxetine, fluvoxamine, metformin, nizatidine, orlistat, phenylpropanolamine, reboxetine, rosiglitazone, sibutramine, topiramate, and metformin+sibutramine. Compared with placebo, metformin had the greatest weight loss (N=7, n=334, -2.94 kg (confidence interval (CI:-4.89,-0.99)), followed by d-fenfluramine (N=1, n=16, -2.60 kg (CI:-5.14,-0.06)), sibutramine (N=2, n=55, -2.56 kg (CI:-3.91,-1.22)), topiramate (N=2, n=133, -2.52 kg (CI:-4.87,-0.16)), and reboxetine (N=2, n=79, -1.90 kg (CI:-3.07,-0.72)). Weight loss remained significant with metformin initiation after weight gain had occurred, but not when started concomitantly with antipsychotics. Nausea rates were not higher with any treatment compared with placebo. In all, 5 of 15 psychopharmacologic interventions aimed at ameliorating antipsychotic-induced weight gain outperformed placebo. Results were most robust for metformin, although these were modest and heterogeneous. Only one (negative) combination treatment study was available and head-to-head studies are absent. None of the agents were able to entirely reverse weight gain because of antipsychotics. At present, no treatment has sufficient evidence to recommend broad clinical usage. Antipsychotics with no or minimal cardiometabolic liability, as well as interventions that prevent or normalize adverse antipsychotic cardiometabolic effects are needed.
Figures
References
-
- Allison DB, Mackell JA, McDonnell DD. The impact of weight gain on quality of life among persons with schizophrenia. Psychiatr Serv. 2003;54:565–567. - PubMed
-
- Allison DB, Mentore JL, Heo M, Chandler LP, Cappelleri JC, Infante MC, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry. 1999;156:1686–1696. - PubMed
-
- Alvarez-Jimenez M, Hetrick SE, Gonzalez-Blanch C, Gleeson JF, McGorry PD. Non-pharmacological management of antipsychotic-induced weight gain: systematic review and meta-analysis of randomised controlled trials. Br J Psychiatry. 2008;193:101–107. - PubMed
-
- Arman S, Sadramely MR, Nadi M, Koleini N. A randomized, double-blind, placebo-controlled trial of metformin treatment for weight gain associated with initiation of risperidone in children and adolescents. Saudi Med J. 2008;29:1130–1134. - PubMed
-
- Assuncao SS, Ruschel SI, Rosa Lde C, Campos JA, Alves MJ, Bracco OL, et al. Weight gain management in patients with schizophrenia during treatment with olanzapine in association with nizatidine. Rev Bras Psiquiatr. 2006;28:270–276. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
