

Prospective assessment of postoperative complications and associated costs following inguinal lymph node dissection (ILND) in melanoma patients
- PMID: 20336388
- PMCID: PMC2943041
- DOI: 10.1245/s10434-010-1026-z
Prospective assessment of postoperative complications and associated costs following inguinal lymph node dissection (ILND) in melanoma patients
Abstract
Background: We prospectively assessed the incidence, risk factors, and costs associated with wound complications and lymphedema in melanoma patients undergoing inguinal lymph node dissection (ILND).
Materials and methods: A total of 53 melanoma patients were accrued to 2 trials (June 2005 to July 2008) that included prospective evaluations of postoperative complications; 30-day wound complications included infection, seroma, and/or dehiscence. There were 20 patients who underwent limb volume measurement and completed a 19-item lymphedema symptom assessment questionnaire preoperatively and 3 months postoperatively. A multivariate analysis was performed to evaluate potential risk factors for complications. A microcosting analysis was also performed to evaluate the direct costs associated with wound complications.
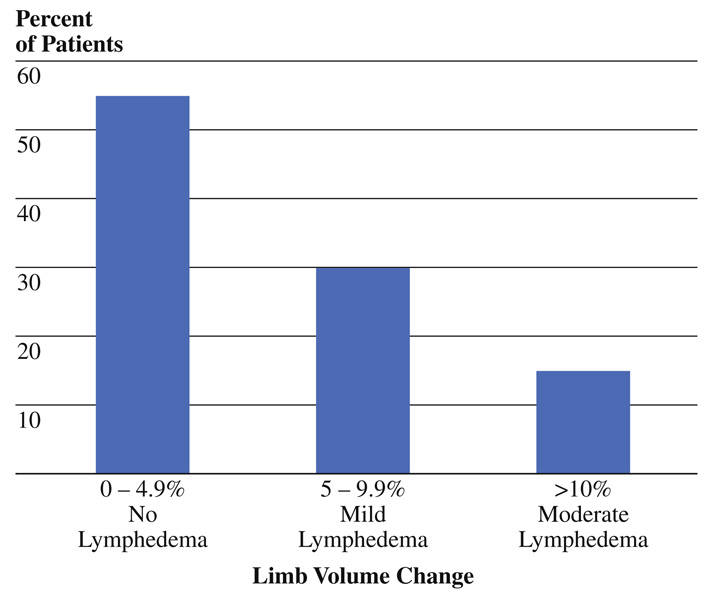
Results: The 30-day wound complications were noted in 77.4% of patients. A BMI ≥ 30 (n = 28) increased the risk for wound complications (odds ratio [OR] = 11.4, 95% confidence interval [95%CI] 1.6-78.5, P = .01), while advanced nodal disease approached significance (OR = 9.0, 95%CI: 0.79-103.1, P = .08). Other risk factors, including diabetes, smoking, and the addition of a deep pelvic (iliac/obturator) dissection to ILND, were not significant. Of 20 patients, 9 (45%) developed limb volume change (LVC) ≥5% at 3 months, with associated mean symptom scores of 6.1 versus 4.6 for those without LVC. Costs for patients with wound complications were significantly higher than for those without wound complications.
Conclusions: Postoperative wound complications and early onset lymphedema occur frequently following ILND for melanoma. Obesity is an adverse risk factor for 30-day wound complications that can significantly increase postoperative costs, as is likely the case for advanced disease. Risk reduction practices and novel treatment approaches are needed to reduce postoperative morbidity.
Figures
References
-
- Hughes TM, Thomas JM. Combined inguinal and pelvic lymph node dissection for stage III melanoma. Br J Surg. 1999;86:1493–1498. - PubMed
-
- Essner R, Scheri R, Kavanagh M, Torisu-Itakura H, Wanek LA, Morton DL. Surgical management of the groin lymph nodes in melanoma in the era of sentinel lymph node dissection. Arch Surg. 2006;141:877–882. discussion 882–4. - PubMed
-
- Hughes TM, A’Hern RP, Thomas JM. Prognosis and surgical management of patients with palpable inguinal lymph node metastases from melanoma. Br J Surg. 2000;87:892–901. - PubMed
-
- Nathansohn N, Schachter J, Gutman H. Patterns of recurrence in patients with melanoma after radical lymph node dissection. Arch Surg. 2005;140:1172–1177. - PubMed
-
- Beitsch P, Balch C. Operative morbidity and risk factor assessment in melanoma patients undergoing inguinal lymph node dissection. Am J Surg. 1992;164:462–465. discussion 465–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
