

Sleep and rhythm consequences of a genetically induced loss of serotonin
- PMID: 20337188
- PMCID: PMC2831424
- DOI: 10.1093/sleep/33.3.307
Sleep and rhythm consequences of a genetically induced loss of serotonin
Abstract
Background: A genetic deficiency in sepiapterin reductase leads to a combined deficit of serotonin and dopamine. The motor phenotype is characterized by a dopa-responsive fluctuating generalized dystonia-parkinsonism. The non-motor symptoms are poorly recognized. In particular, the effects of brain serotonin deficiency on sleep have not been thoroughly studied.
Objective: We examine the sleep, sleep-wake rhythms, CSF neurotransmitters, and melatonin profile in a patient with sepiapterin reductase deficiency.
Patient: The patient was a 28-year-old man with fluctuating generalized dystonia-parkinsonism caused by sepiapterin reductase deficiency.
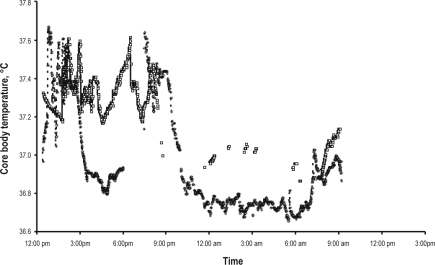
Methods: A sleep interview, wrist actigraphy, sleep log over 14 days, 48-h continuous sleep and core temperature monitoring, and measurement of CSF neurotransmitters and circadian serum melatonin and cortisol levels before and after treatment with 5-hydroxytryptophan (the precursor of serotonin) and levodopa were performed.
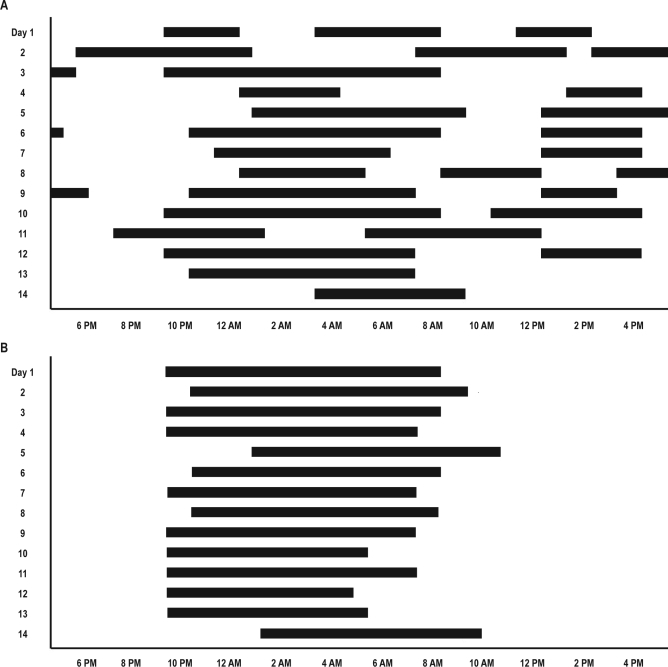
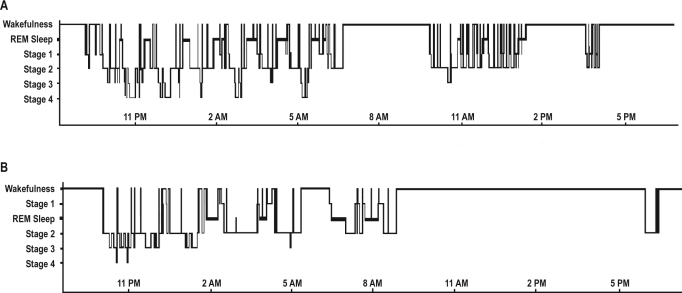
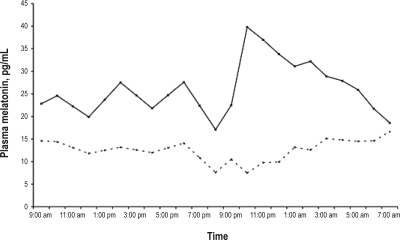
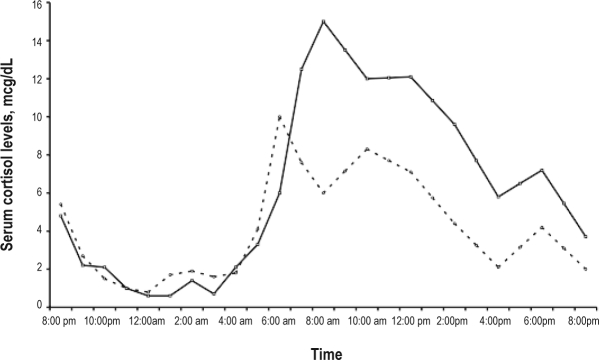
Results: Before treatment, the patient had mild hypersomnia with long sleep time (704 min), ultradian sleep-wake rhythm (sleep occurred every 11.8 +/- 5.3 h), organic hyperphagia, attentionlexecutive dysfunction, and no depression. The serotonin metabolism in the CSF was reduced, and the serum melatonin profile was flat, while cortisol and core temperature profiles were normal. Supplementation with 5-hydroxytryptophan, but not with levodopa, normalized serotonin metabolism in the CSF, reduced sleep time to 540 min, normalized the eating disorder and the melatonin profile, restored a circadian sleep-wake rhythm (sleep occurred every 24 +/- 1.7 h, P < 0.0001), and improved cognition.
Conclusion: In this unique genetic paradigm, the melatonin deficiency (caused by a lack of its substrate, serotonin) may cause the ultradian sleep-wake rhythm.
Figures

Similar articles
-
Dopa-responsive hypersomnia and mixed movement disorder due to sepiapterin reductase deficiency.Neurology. 2006 Dec 12;67(11):2032-5. doi: 10.1212/01.wnl.0000247274.21261.b4. Neurology. 2006. PMID: 17159114
-
Sepiapterin reductase deficiency an autosomal recessive DOPA-responsive dystonia.Mol Genet Metab. 2006 Sep-Oct;89(1-2):116-20. doi: 10.1016/j.ymgme.2006.03.010. Epub 2006 May 2. Mol Genet Metab. 2006. PMID: 16650784
-
Circadian Melatonin and Temperature Taus in Delayed Sleep-wake Phase Disorder and Non-24-hour Sleep-wake Rhythm Disorder Patients: An Ultradian Constant Routine Study.J Biol Rhythms. 2016 Aug;31(4):387-405. doi: 10.1177/0748730416650069. Epub 2016 Jun 16. J Biol Rhythms. 2016. PMID: 27312974
-
Precision medicine in circadian rhythm sleep-wake disorders: current state and future perspectives.Per Med. 2017 Mar;14(2):171-182. doi: 10.2217/pme-2016-0079. Epub 2017 Jan 24. Per Med. 2017. PMID: 29754559 Review.
-
Drugs Used in Circadian Sleep-Wake Rhythm Disturbances.Sleep Med Clin. 2020 Jun;15(2):301-310. doi: 10.1016/j.jsmc.2020.02.015. Sleep Med Clin. 2020. PMID: 32386703 Review.
Cited by
-
Genotype-phenotype correlations in sepiapterin reductase deficiency. A splicing defect accounts for a new phenotypic variant.Neurogenetics. 2011 Aug;12(3):183-91. doi: 10.1007/s10048-011-0279-4. Epub 2011 Mar 24. Neurogenetics. 2011. PMID: 21431957
-
Sleep and sleep disorders in rare hereditary diseases: a reminder for the pediatrician, pediatric and adult neurologist, general practitioner, and sleep specialist.Front Neurol. 2014 Jul 17;5:133. doi: 10.3389/fneur.2014.00133. eCollection 2014. Front Neurol. 2014. PMID: 25101051 Free PMC article. Review.
-
Simultaneous determination of all forms of biopterin and neopterin in cerebrospinal fluid.ACS Chem Neurosci. 2014 Jul 16;5(7):533-41. doi: 10.1021/cn4001928. Epub 2014 Apr 8. ACS Chem Neurosci. 2014. PMID: 24650440 Free PMC article.
-
Neurobiology, pathophysiology, and treatment of melatonin deficiency and dysfunction.ScientificWorldJournal. 2012;2012:640389. doi: 10.1100/2012/640389. Epub 2012 May 2. ScientificWorldJournal. 2012. PMID: 22629173 Free PMC article. Review.
-
Sleep, cerebrospinal fluid, and the glymphatic system: A systematic review.Sleep Med Rev. 2022 Feb;61:101572. doi: 10.1016/j.smrv.2021.101572. Epub 2021 Nov 18. Sleep Med Rev. 2022. PMID: 34902819 Free PMC article.
References
-
- Blau N, Bonafé L, Thö B. Tetrahydrobiopterin deficiencies without hyperphenylalaninemia: diagnosis and genetics of dopa–responsive dystonia and sepiapterin reductase deficiency. Mol Genet Metab. 2001;74:172–85. - PubMed
-
- Neville BG, Parascandalo R, Farrugia R, Felice A. Sepiapterin reductase deficiency: a congenital dopa–responsive motor and cognitive disorder. Brain. 2005;128:2291–6. - PubMed
-
- Abeling NG, Duran M, Bakker HD, et al. Sepiapterin reductase deficiency an autosomal recessive DOPA–responsive dystonia. Mol Genet Metab. 2006;89:116–20. - PubMed
-
- Echenne B, Roubertie A, Assmann B, et al. Sepiapterin reductase deficiency: clinical presentation and evaluation of long–term therapy. Pediatr Neurol. 2006;35:308–13. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
