

The prevalence of stunting, overweight and obesity, and metabolic disease risk in rural South African children
- PMID: 20338024
- PMCID: PMC2853509
- DOI: 10.1186/1471-2458-10-158
The prevalence of stunting, overweight and obesity, and metabolic disease risk in rural South African children
Abstract
Background: Low- to middle-income countries are undergoing a health transition with non-communicable diseases contributing substantially to disease burden, despite persistence of undernutrition and infectious diseases. This study aimed to investigate the prevalence and patterns of stunting and overweight/obesity, and hence risk for metabolic disease, in a group of children and adolescents in rural South Africa.
Methods: A cross-sectional growth survey was conducted involving 3511 children and adolescents 1-20 years, selected through stratified random sampling from a previously enumerated population living in Agincourt sub-district, Mpumalanga Province, South Africa. Anthropometric measurements including height, weight and waist circumference were taken using standard procedures. Tanner pubertal assessment was conducted among adolescents 9-20 years. Growth z-scores were generated using 2006 WHO standards for children up to five years and 1977 NCHS/WHO reference for older children. Overweight and obesity for those <18 years were determined using International Obesity Task Force BMI cut-offs, while adult cut-offs of BMI > or = 25 and > or = 30 kg/m2 for overweight and obesity respectively were used for those > or = 18 years. Waist circumference cut-offs of > or = 94 cm for males and > or = 80 cm for females and waist-to-height ratio of 0.5 for both sexes were used to determine metabolic disease risk in adolescents.
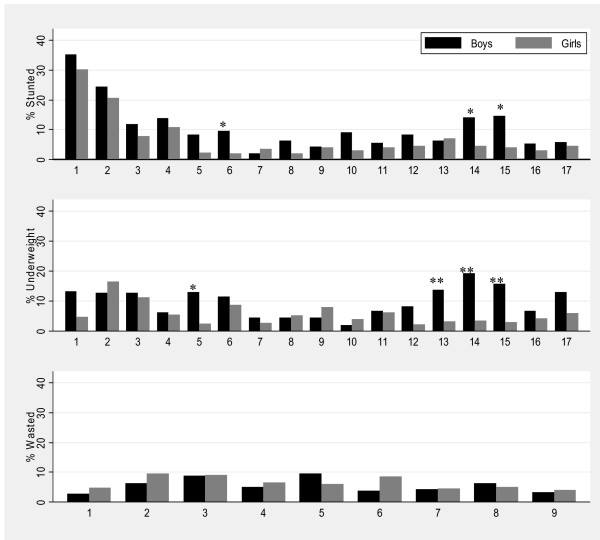
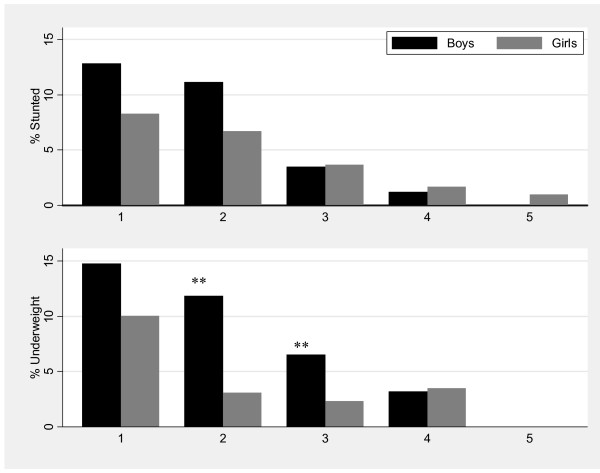
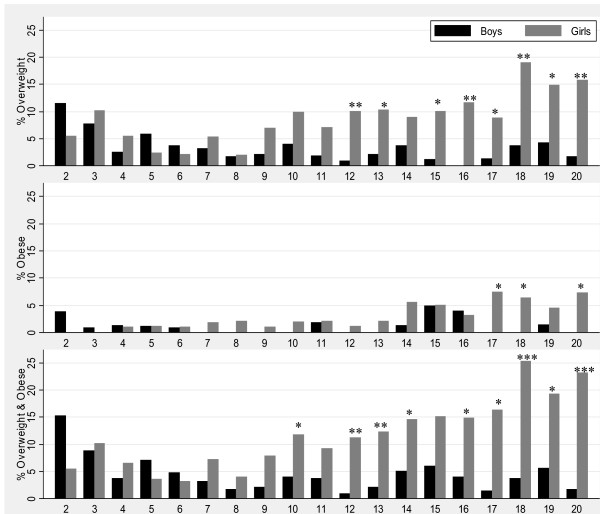
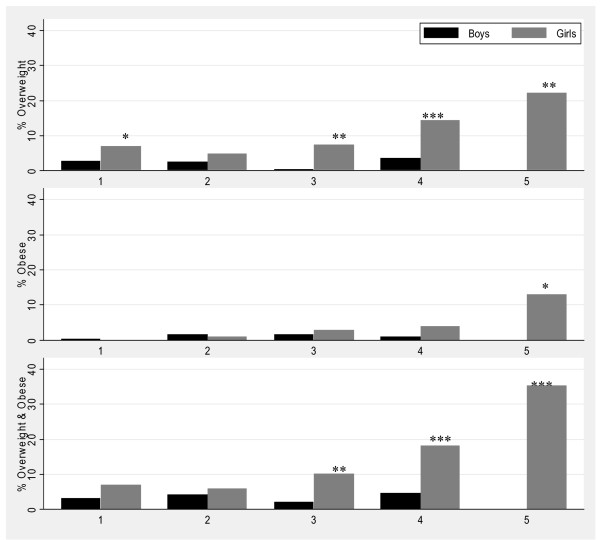
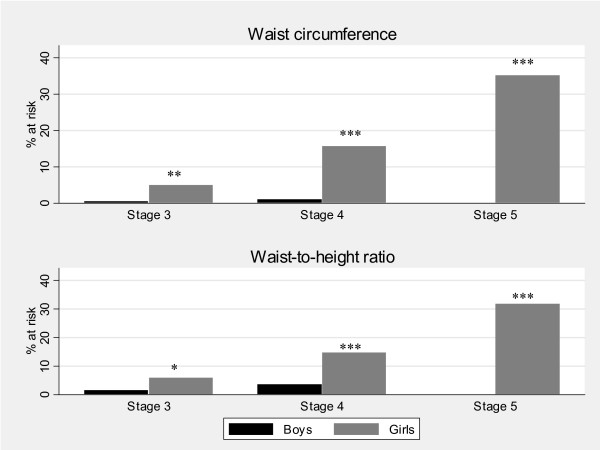
Results: About one in five children aged 1-4 years was stunted; one in three of those aged one year. Concurrently, the prevalence of combined overweight and obesity, almost non-existent in boys, was substantial among adolescent girls, increasing with age and reaching approximately 20-25% in late adolescence. Central obesity was prevalent among adolescent girls, increasing with sexual maturation and reaching a peak of 35% at Tanner Stage 5, indicating increased risk for metabolic disease.
Conclusions: The study highlights that in transitional societies, early stunting and adolescent obesity may co-exist in the same socio-geographic population. It is likely that this profile relates to changes in nutrition and diet, but variation in factors such as infectious disease burden and physical activity patterns, as well as social influences, need to be investigated. As obesity and adult short stature are risk factors for metabolic syndrome and Type 2 diabetes, this combination of early stunting and adolescent obesity may be an explosive combination.
Figures
References
-
- World Health Organization. World Health Report 2002: Reducing Risks, Promoting Healthy Life. WHO, Geneva; 2002.
-
- Lanigan J, Singhal A. Early nutrition and long-term health: a practical approach. Proc Nutr Soc. 2009. pp. 1–8. - PubMed
-
- Food and Agriculture Organization (FAO) of the United Nations. The double burden of malnutrition Case studies from six developing countries. FAO food and nutrition paper 84. Rome; 2006. - PubMed
-
- Popkin B. The Nutrition Transition in the Developing World. Dev Policy Rev. 2003;21(5-6):581–597. doi: 10.1111/j.1467-8659.2003.00225.x. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
