

Scope and impact of early and late preterm infants admitted to the PICU with respiratory illness
- PMID: 20338574
- PMCID: PMC2892737
- DOI: 10.1016/j.jpeds.2010.02.006
Scope and impact of early and late preterm infants admitted to the PICU with respiratory illness
Abstract
Objective: To determine the clinical course and outcomes of children born early preterm (EPT, <32 weeks), late preterm (LPT, 32 to 35 weeks), and full term (FT, >or=36 weeks) who were subsequently admitted to the pediatric intensive care unit (PICU) with respiratory illness.
Study design: Retrospective chart review of patients <2 years old admitted to a tertiary PICU with respiratory illness.
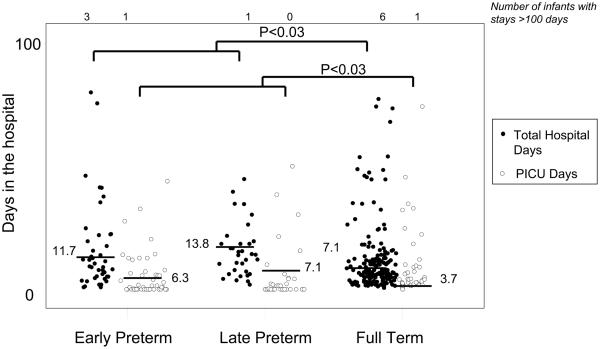
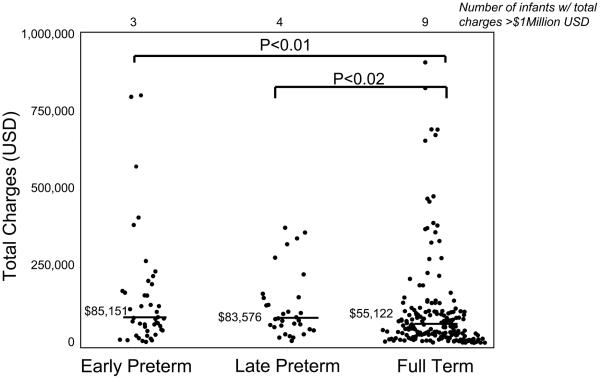
Results: Two hundred seventy-one patients met inclusion criteria: 17.3% were EPT, 12.2% were LPT, and 70.5% were FT. Lower respiratory tract infection was the most common diagnosis (55%) for all groups. Median PICU length of stay was longer for EPT (6.3 days) and LPT infants (7.1 days) compared with FT infants (3.7 days; P < .03 for both comparisons). EPT and LPT infants had longer hospital stays (median, 11.7 and 13.8 days, respectively) compared with FT infants (median, 7.1 days; P < .03 and P = .004, respectively). Median hospital charges were also greater for EPT ($85 151) and LPT ($83 576) groups compared with FT group ($55 122; P < .01 and P < .02, respectively).
Conclusions: EPT and LPT infants comprise a considerable proportion of PICU admissions for respiratory illness and have greater resource utilization than FT infants.
Copyright (c) 2010 Mosby, Inc. All rights reserved.
Figures
References
-
- Gregoire MC, Lefebvre F, Glorieux J. Health and developmental outcomes at 18 months in very preterm infants with bronchopulmonary dysplasia. Pediatrics. 1998 May;101:856–60. - PubMed
-
- Furman L, Baley J, Borawski-Clark E, Aucott S, Hack M. Hospitalization as a measure of morbidity among very low birth weight infants with chronic lung disease. J Pediatr. 1996 Apr;128:447–52. - PubMed
-
- Gross SJ, Iannuzzi DM, Kveselis DA, Anbar RD. Effect of preterm birth on pulmonary function at school age: a prospective controlled study. J Pediatr. 1998 Aug;133:188–92. - PubMed
-
- Smith VC, Zupancic JA, McCormick MC, Croen LA, Greene J, Escobar GJ, et al. Rehospitalization in the first year of life among infants with bronchopulmonary dysplasia. J Pediatr. 2004 Jun;144:799–803. - PubMed
-
- Prais D, Schonfeld T, Amir J. Admission to the intensive care unit for respiratory syncytial virus bronchiolitis: a national survey before palivizumab use. Pediatrics. 2003 Sep;112:548–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
