

Lung transplant airway hypoxia: a diathesis to fibrosis?
- PMID: 20339145
- PMCID: PMC3269232
- DOI: 10.1164/rccm.200910-1573OC
Lung transplant airway hypoxia: a diathesis to fibrosis?
Abstract
Rationale: Chronic rejection, manifested pathologically as airway fibrosis, is the major problem limiting long-term survival in lung transplant recipients. Airway hypoxia and ischemia, resulting from a failure to restore the bronchial artery (BA) circulation at the time of transplantation, may predispose patients to chronic rejection. To address this possibility, clinical information is needed describing the status of lung perfusion and airway oxygenation after transplantation.
Objectives: To determine the relative pulmonary arterial blood flow, airway tissue oxygenation and BA anatomy in the transplanted lung was compared with the contralateral native lung in lung allograft recipients.
Methods: Routine perfusion scans were evaluated at 3 and 12 months after transplantation in 15 single transplant recipients. Next, airway tissue oximetry was performed in 12 patients during surveillance bronchoscopies in the first year after transplant and in 4 control subjects. Finally, computed tomography (CT)-angiography studies on 11 recipients were reconstructed to evaluate the post-transplant anatomy of the BAs.
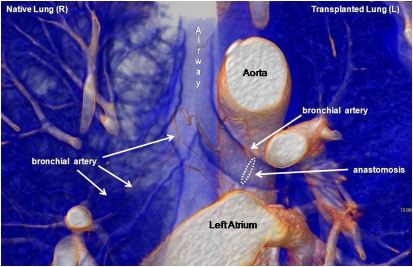
Measurements and main results: By 3 months after transplantation, deoxygenated pulmonary arterial blood is shunted away from the native lung to the transplanted lung. In the first year, healthy lung transplant recipients exhibit significant airway hypoxia distal to the graft anastomosis. CT-angiography studies demonstrate that BAs are abbreviated, generally stopping at or before the anastomosis, in transplant airways.
Conclusions: Despite pulmonary artery blood being shunted to transplanted lungs after transplantation, grafts are hypoxic compared with both native (diseased) and control airways. Airway hypoxia may be due to the lack of radiologically demonstrable BAs after lung transplantation.
Figures
Comment in
-
Airway hypoxia, bronchiolar artery revascularization, and obliterative bronchiolitis/bronchiolitis obliterans syndrome: are we there yet?Am J Respir Crit Care Med. 2010 Jul 15;182(2):136-7. doi: 10.1164/rccm.201004-0508ED. Am J Respir Crit Care Med. 2010. PMID: 20634500 No abstract available.
References
-
- Luckraz H, Goddard M, McNeil K, Atkinson C, Charman SC, Stewart S, Wallwork J. Microvascular changes in small airways predispose to obliterative bronchiolitis after lung transplantation. J Heart Lung Transplant 2004;23:527–531. - PubMed
-
- Luckraz H, Goddard M, McNeil K, Atkinson C, Sharples LD, Wallwork J. Is obliterative bronchiolitis in lung transplantation associated with microvascular damage to small airways? Ann Thorac Surg 2006;82:1212–1218. - PubMed
-
- Ishii Y, Sawada T, Kubota K, Fuchinoue S, Teraoka S, Shimizu A. Injury and progressive loss of peritubular capillaries in the development of chronic allograft nephropathy. Kidney Int 2005;67:321–332. - PubMed
-
- Ozdemir BH, Demirhan B, Ozdemir FN, Dalgic A, Haberal M. The role of microvascular injury on steroid and OKT3 response in renal allograft rejection. Transplantation 2004;78:734–740. - PubMed
-
- Labarrere CA, Nelson DR, Park JW. Pathologic markers of allograft arteriopathy: insight into the pathophysiology of cardiac allograft chronic rejection. Curr Opin Cardiol 2001;16:110–117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
