

An aggressive approach leads to improved survival in hepatocellular carcinoma patients with portal vein tumor thrombus
- PMID: 20340033
- PMCID: PMC3015200
- DOI: 10.1007/s00432-010-0868-x
An aggressive approach leads to improved survival in hepatocellular carcinoma patients with portal vein tumor thrombus
Abstract
Purpose: Many physicians express a relatively nihilistic approach to the treatment of hepatocellular carcinoma (HCC) with portal vein tumor thrombus (PVTT). Consensus among surgeons regarding the indications for an aggressive approach has not been reached. Current study was aimed to determine whether an aggressive approach, with an extended resection with thrombectomy and adjuvant therapy, would lead to an improved survival for HCC patients with PVTT.
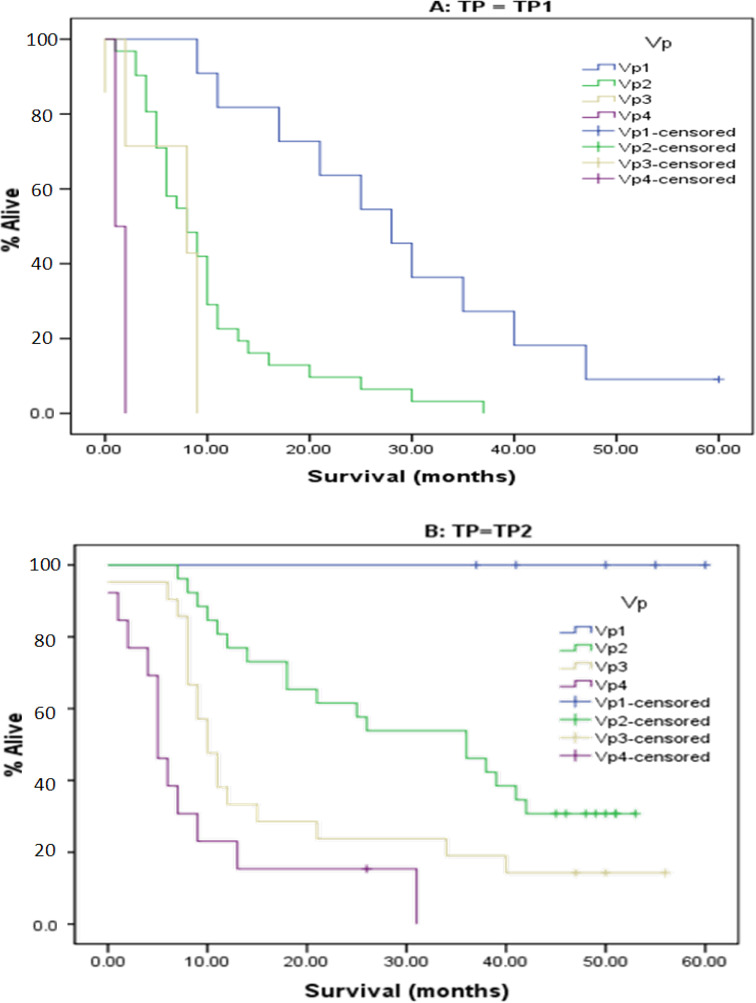
Methods: A retrospective review of 116 HCC patients with PVTT admitted from 1996 to 2006 was conducted. Patients were divided into 2 time-period (TP) cohorts, of them, 51 cases in the first 5 years (TP1) and 65 in the last 5 years (TP2).
Results: Surgical operations were performed on 68 patients. Twenty-one surgical resections were performed in TP1 and forty-seven in TP2. The extent of liver resections, as well as the frequency of thrombectomy, was greater in TP2 (P = 0.039). During both time-periods, an aggressive therapy was associated with improved survival (P < 0.02 TP1, P < 0.001 TP2). Overall survival of all patients in TP2 was significantly greater than in TP1 (P < 0.001), with a median survival of 15 months in TP2, whereas in TP1, the survival was only 9 months. The median 1-, 3-year survivals in TP2 (54 and 34%, respectively) were also greater than that in TP1 (31 and 7%, respectively). A multiple logistic regression analysis revealed that radical resection and adjuvant therapy were the independent predictors of overall survival.
Conclusions: An aggressive approach, combining extended liver resection with thrombectomy and adjuvant therapy, leads to an improved survival in the HCC patients with PVTT.
Figures



References
-
- Chung JW, Park JH, Han JK, Choi BI, Han MC (1995) Hepatocellular carcinoma and portal vein invasion: results of treatment with transcatheter oily chemoembolization. AJR Am J Roentgenol 165(2):315–321 - PubMed
-
- Couinaud C (1994) Intrahepatic anatomy. Application to liver transplantation. Ann Radiol (Paris) 37(5):323–333 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
