

Measures of site resourcing predict virologic suppression, immunologic response and HIV disease progression following highly active antiretroviral therapy (HAART) in the TREAT Asia HIV Observational Database (TAHOD)
- PMID: 20345881
- PMCID: PMC2914850
- DOI: 10.1111/j.1468-1293.2010.00822.x
Measures of site resourcing predict virologic suppression, immunologic response and HIV disease progression following highly active antiretroviral therapy (HAART) in the TREAT Asia HIV Observational Database (TAHOD)
Abstract
Objectives: Surrogate markers of HIV disease progression are HIV RNA in plasma viral load (VL) and CD4 cell count (immune function). Despite improved international access to antiretrovirals, surrogate marker diagnostics are not routinely available in resource-limited settings. Therefore, the objective was to assess effects of economic and diagnostic resourcing on patient treatment outcomes.
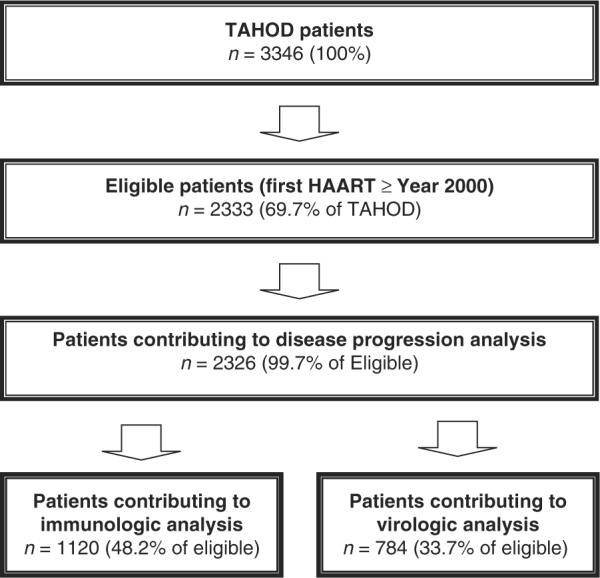
Methods: Analyses were based on 2333 patients initiating highly active antiretroviral therapy (HAART) from 2000 onwards. Sites were categorized by World Bank country income criteria (high/low) and annual frequency of VL (> or = 3, 1-2 or <1) or CD4 (> or = 3 or <3) testing. Endpoints were time to AIDS/death and change in CD4 cell count and VL suppression (<400 HIV-1 RNA copies/mL) at 12 months. Demographics, Centers for Disease Control and Prevention (CDC) classification, baseline VL/CD4 cell counts, hepatitis B/C coinfections and HAART regimen were covariates. Time to AIDS/death was analysed by proportional hazards models. CD4 and VL endpoints were analysed using linear and logistic regression, respectively.
Results: Increased disease progression was associated with site-reported VL testing less than once per year [hazard ratio (HR)=1.4; P=0.032], severely symptomatic HIV infection (HR=1.4; P=0.003) and hepatitis C virus coinfection (HR=1.8; P=0.011). A total of 1120 patients (48.2%) had change in CD4 cell count data. Smaller increases were associated with older age (P<0.001) and 'Other' HIV source exposures, including injecting drug use and blood products (P=0.043). A total of 785 patients (33.7%) contributed to the VL suppression analyses. Patients from sites with VL testing less than once per year [odds ratio (OR)=0.30; P<0.001] and reporting 'Other' HIV exposures experienced reduced suppression (OR=0.28; P<0.001).
Conclusion: Low measures of site resourcing were associated with less favourable patient outcomes, including a 35% increase in disease progression in patients from sites with VL testing less than once per year.
Figures
References
-
- UNAIDS AIDS epidemic update: special report on HIV/AIDS. 2006. Available at www.unaids.org/en/KnowledgeCentre/HIVData/EpiUpdate/EpiUpdArchive/2006/d....
-
- Egger M, Boulle A, Schechter M, Miotti P. Antiretroviral therapy in resource-poor settings: scaling up inequalities? Int J Epidemiol. 2005;34:509–512. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
