

Cost of acute renal replacement therapy in the intensive care unit: results from The Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) study
- PMID: 20346163
- PMCID: PMC2887158
- DOI: 10.1186/cc8933
Cost of acute renal replacement therapy in the intensive care unit: results from The Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) study
Abstract
Introduction: Severe acute kidney injury (AKI) can be treated with either continuous renal replacement therapy (CRRT) or intermittent renal replacement therapy (IRRT). Limited evidence from existing studies does not support an outcome advantage of one modality versus the other, and most centers around the word use both modalities according to patient needs. However, cost estimates involve multiple factors that may not be generalizable to other sites, and, to date, only single-center cost studies have been performed. The aim of this study was to estimate the cost difference between CRRT and IRRT in the intensive care unit (ICU).
Methods: We performed a post hoc analysis of a prospective observational study among 53 centers from 23 countries, from September 2000 to December 2001. We estimated costs based on staffing, as well as dialysate and replacement fluid, anticoagulation and extracorporeal circuit.
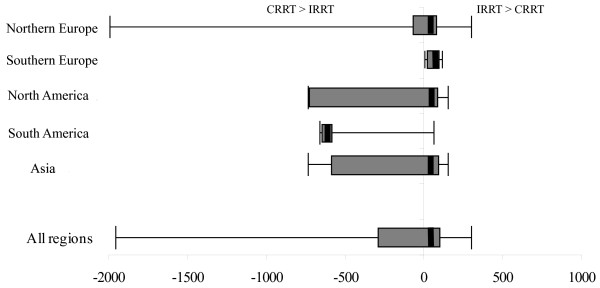
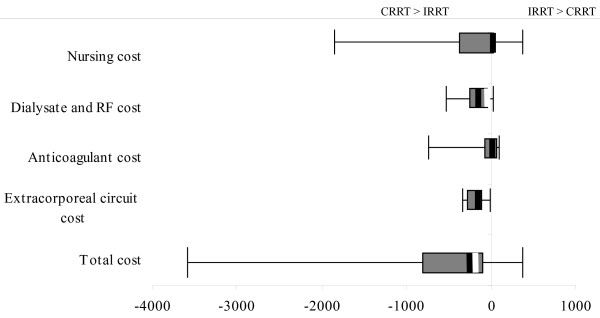
Results: We found that the theoretic range of costs were from $3,629.80/day more with CRRT to $378.60/day more with IRRT. The median difference in cost between CRRT and IRRT was $289.60 (IQR 830.8-116.8) per day (greater with CRRT). Costs also varied greatly by region. Reducing replacement fluid volumes in CRRT to <or= 25 ml/min (approximately 25 ml/kg/hr) would result in $67.20/day (23.2%) mean savings.
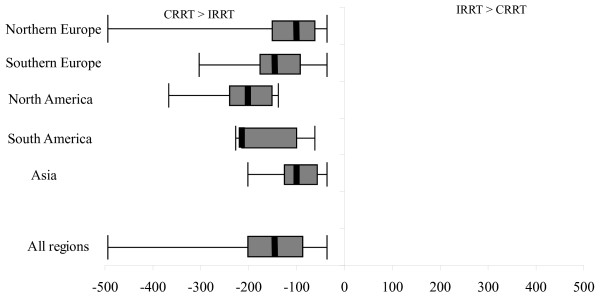
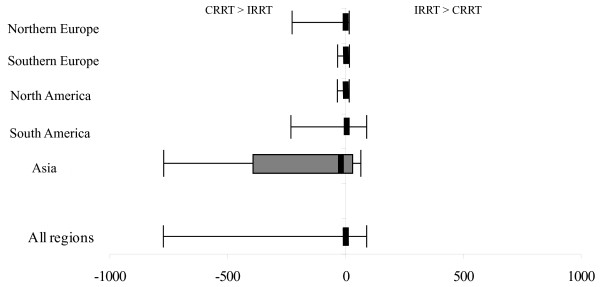
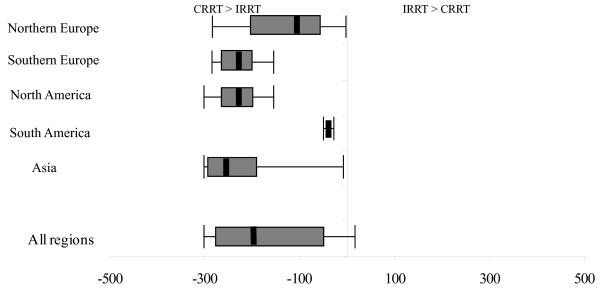
Conclusions: Cost considerations with RRT are important and vary substantially among centers. We identified the relative impact of four cost domains (nurse staffing, fluid, anticoagulation, and extracorporeal circuit) on overall cost differences, and hospitals can look to these areas to reduce costs associated with RRT.
Figures
References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C. for the Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. doi: 10.1001/jama.294.7.813. - DOI - PubMed
-
- Bellomo R, Farmer M, Bhonagiri S, Porceddu S, Ariens M, M'Pisi D, Ronco C. Changing acute renal failure treatment from intermittent hemodialysis to continuous hemofiltration: impact on azotemic control. Int J Artif Organs. 1999;22:145–150. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
