

Perioperative infusion of low- dose of vasopressin for prevention and management of vasodilatory vasoplegic syndrome in patients undergoing coronary artery bypass grafting-A double-blind randomized study
- PMID: 20346182
- PMCID: PMC2855562
- DOI: 10.1186/1749-8090-5-17
Perioperative infusion of low- dose of vasopressin for prevention and management of vasodilatory vasoplegic syndrome in patients undergoing coronary artery bypass grafting-A double-blind randomized study
Abstract
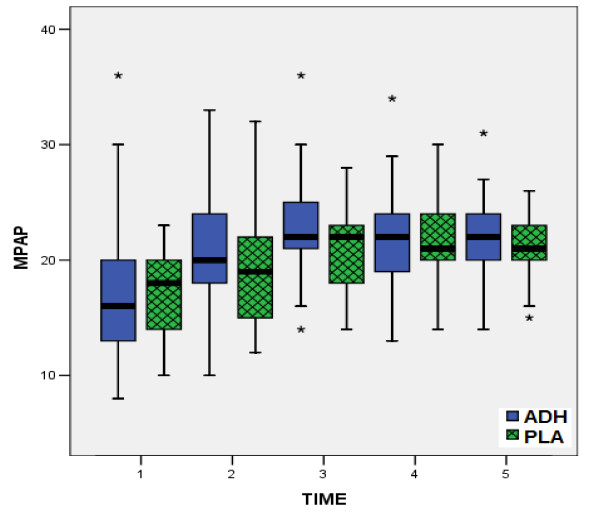
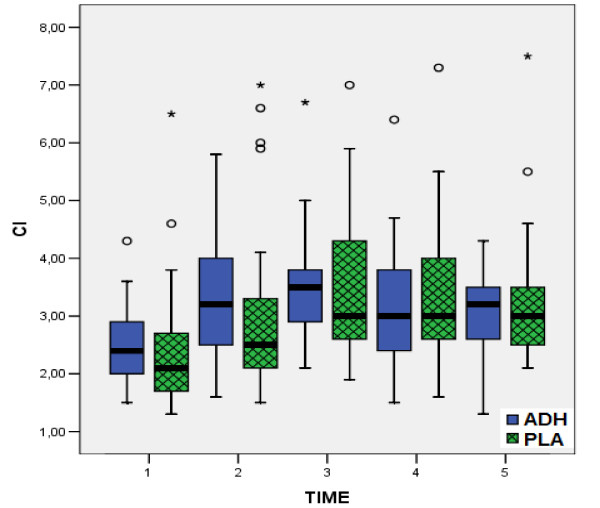
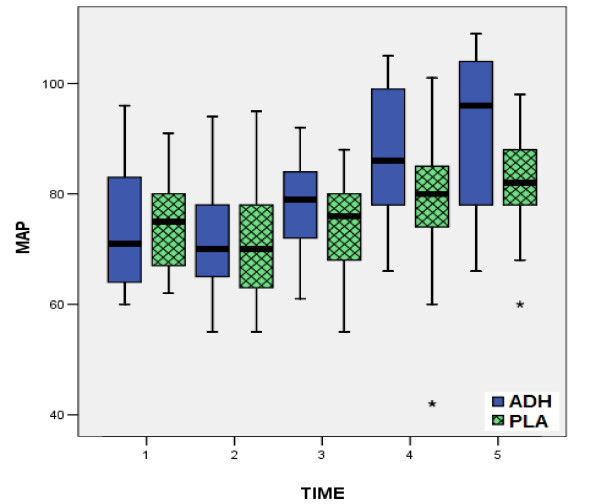
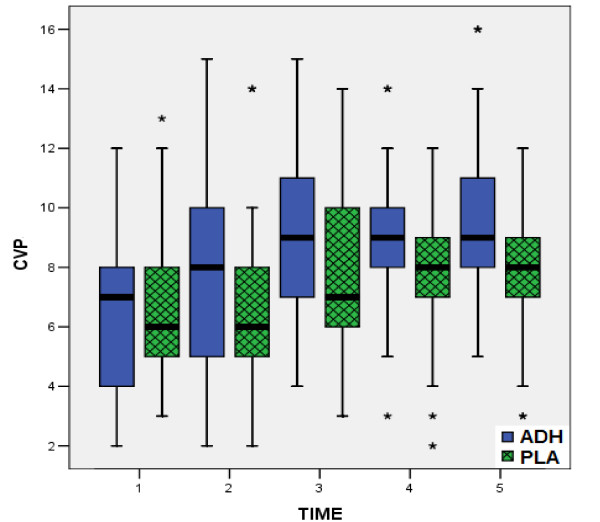
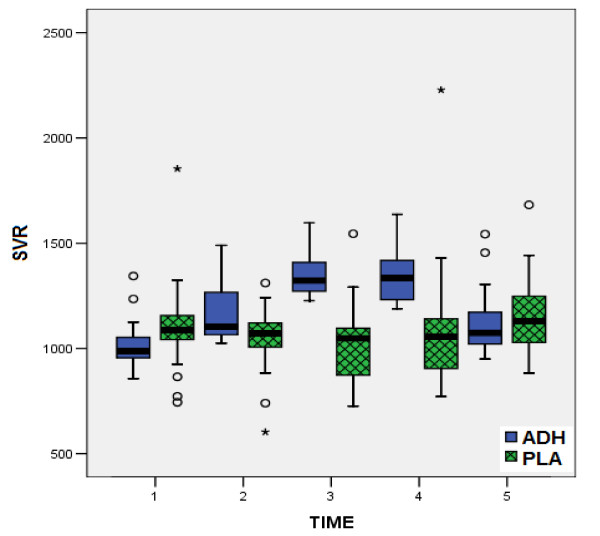
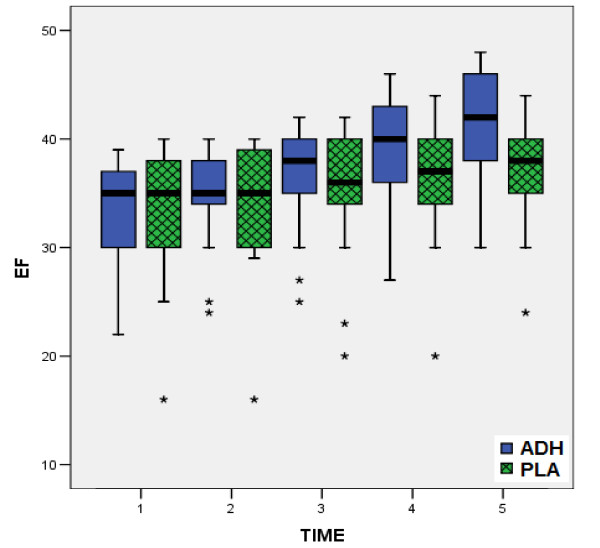
Preoperative medication by inhibitors of angiotensin-converting enzyme (ACE) in coronary artery patients predisposes to vasoplegic shock early after coronary artery bypass grafting. Although in the majority of the cases this shock is mild, in some of them it appears as a situation, "intractable" to high-catecholamine dose medication. In this study we examined the possible role of prophylactic infusion of low-dose vasopressin, during and for the four hours post-bypass after cardiopulmonary bypass, in an effort to prevent this syndrome. In addition, we studied the influence of infused vasopressin on the hemodynamics of the patients, as well as on the postoperative urine-output and blood-loss. In our study 50 patients undergoing coronary artery bypass grafting were included in a blind-randomized basis. Two main criteria were used for the eligibility of patients for coronary artery bypass grafting: ejection fraction between 30-40%, and patients receiving ACE inhibitors, at least for four weeks preoperatively. The patients were randomly divided in two groups, the group A who were infused with 0.03 IU/min vasopressin and the group B who were infused with normal saline intraoperativelly and for the 4 postoperative hours. Measurements of mean artery pressure (MAP), central venous pressure (CVP), systemic vascular resistance (SVR), ejection fracture (EF), heart rate (HR), mean pulmonary artery pressure (MPAP), cardiac index (CI) and pulmonary vascular resistance (PVR) were performed before, during, and after the operation. The requirements of catecholamine support, the urine-output, the blood-loss, and the requirements in blood, plasma and platelets for the first 24 hours were included in the data collected. The incidence of vasodilatory shock was significantly lower (8% vs 20%) in group A and B respectively (p = 0,042). Generally, the mortality was 12%, exclusively deriving from group B. Postoperatively, significant higher values of MAP, CVP, SVR and EF were recorded in the patients of group A, compared to those of group B. In group A norepinephrine was necessary in fewer patients (p = 0.002) and with a lower mean dose (p = 0.0001), additive infusion of epinephrine was needed in fewer patients (p = 0.001), while both were infused for a significant shorter infusion-period (p = 0.0001). Vasopressin administration (for group A) was associated with a higher 24 hour diuresis) (0.0001).In conclusion, low-dose of infused vasopressin during cardiopulmonary bypass and for the next 4 hours is beneficial for its postoperative hemodynamic profile, reduces the doses of requirements of catecholamines and contributes to prevention of the postcardiotomy vasoplegic shock in the patient with low ejection fraction who is receiving ACE preoperatively.
Figures
References
-
- Noto A, Lentini S, Versaci A, Giardina M, Risitano DC, Messina R, David A. A retrospective analysis of terlipressin in bolus for the management of refractory vasoplegic hypotension after cardiac surgery. Interact CardioVascular and Thoracic Surgery. 2009;9:588–92. doi: 10.1510/icvts.2009.209890. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
