

Analysis of the effectiveness of interventions used during the 2009 A/H1N1 influenza pandemic
- PMID: 20346187
- PMCID: PMC2853510
- DOI: 10.1186/1471-2458-10-168
Analysis of the effectiveness of interventions used during the 2009 A/H1N1 influenza pandemic
Abstract
Background: Following the emergence of the A/H1N1 2009 influenza pandemic, public health interventions were activated to lessen its potential impact. Computer modelling and simulation can be used to determine the potential effectiveness of the social distancing and antiviral drug therapy interventions that were used at the early stages of the pandemic, providing guidance to public health policy makers as to intervention strategies in future pandemics involving a highly pathogenic influenza strain.
Methods: An individual-based model of a real community with a population of approximately 30,000 was used to determine the impact of alternative interventions strategies, including those used in the initial stages of the 2009 pandemic. Different interventions, namely school closure and antiviral strategies, were simulated in isolation and in combination to form different plausible scenarios. We simulated epidemics with reproduction numbers R0 of 1.5, which aligns with estimates in the range 1.4-1.6 determined from the initial outbreak in Mexico.
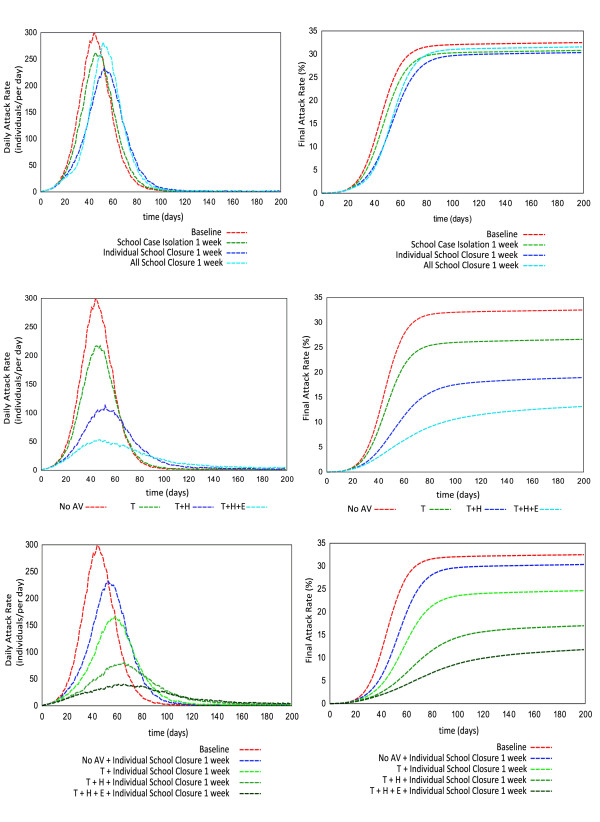
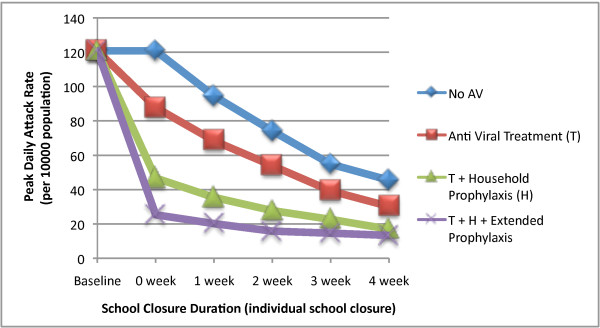
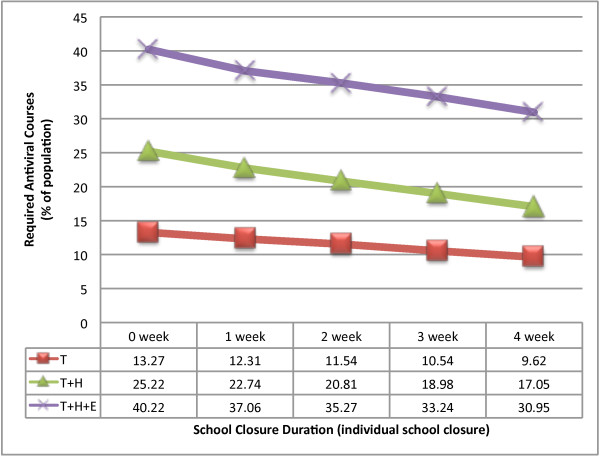
Results: School closure of 1 week was determined to have minimal effect on reducing overall illness attack rate. Antiviral drug treatment of 50% of symptomatic cases reduced the attack rate by 6.5%, from an unmitigated rate of 32.5% to 26%. Treatment of diagnosed individuals combined with additional household prophylaxis reduced the final attack rate to 19%. Further extension of prophylaxis to close contacts (in schools and workplaces) further reduced the overall attack rate to 13% and reduced the peak daily illness rate from 120 to 22 per 10,000 individuals. We determined the size of antiviral stockpile required; the ratio of the required number of antiviral courses to population was 13% for the treatment-only strategy, 25% for treatment and household prophylaxis and 40% for treatment, household and extended prophylaxis. Additional simulations suggest that coupling school closure with the antiviral strategies further reduces epidemic impact.
Conclusions: These results suggest that the aggressive use of antiviral drugs together with extended school closure may substantially slow the rate of influenza epidemic development. These strategies are more rigorous than those actually used during the early stages of the relatively mild 2009 pandemic, and are appropriate for future pandemics that have high morbidity and mortality rates.
Figures


References
-
- WHO: Pandemic (H1N1) 2009 - update 87. http://www.who.int/csr/don/2010_02_12/en/index.html
-
- Australian Commonwealth Department of Health and Aging: Pandemic (H1N1) 2009 update bulletins for 7 to 13 September 2009. http://www.healthemergency.gov.au/internet/healthemergency/publishing.ns...
-
- Australian Commonwealth Department of Health and Aging: Australian Health Management Plan for Pandemic Influenza. http://www.flupandemic.gov.au/internet/panflu/publishing.nsf/Content/ahm...
-
- US Department of Health and Human Services: Pandemic Influenza Plan. http://www.hhs.gov/pandemicflu/plan/
-
- United Kingdom Department of Health: Pandemic flu: A national framework for responding to an influenza pandemic. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicati...
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
