

Irradiation of pediatric high-grade spinal cord tumors
- PMID: 20346593
- PMCID: PMC5095924
- DOI: 10.1016/j.ijrobp.2009.09.071
Irradiation of pediatric high-grade spinal cord tumors
Abstract
Purpose: To report the outcome using radiation therapy (RT) for pediatric patients with high-grade spinal cord tumors.
Methods and materials: A retrospective chart review was conducted that included 17 children with high-grade spinal cord tumors treated with RT at St. Jude Children's Research Hospital between 1981 and 2007. Three patients had gross total resection, 11 had subtotal resection, and 3 underwent biopsy. The tumor diagnosis was glioblastoma multiforme (n = 7), anaplastic astrocytoma (n = 8), or anaplastic oligodendroglioma (n = 2). Seven patients received craniospinal irradiation (34.2-48.6 Gy). The median dose to the primary site was 52.2 Gy (range, 38-66 Gy).
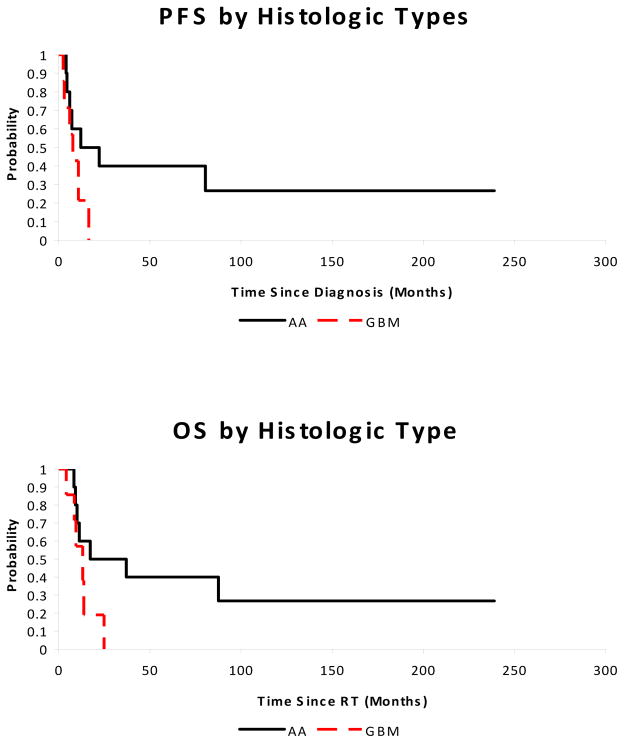
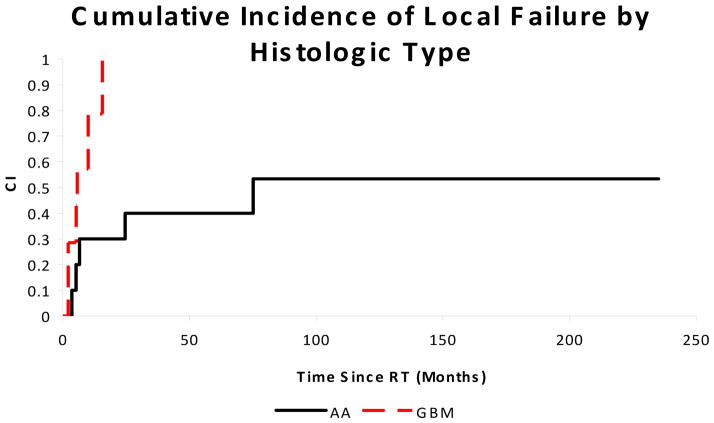
Results: The median progression-free and overall survivals were 10.8 and 13.8 months, respectively. Local tumor progression at 12 months (79% vs. 30%, p = 0.02) and median survival (13.1 vs. 27.2 months, p = 0.09) were worse for patients with glioblastoma multiforme compared with anaplastic astrocytoma or oligodendroglioma. The median overall survival was shorter for patients when failure included neuraxis dissemination (n = 8) compared with local failure alone (n = 5), 9.6 vs. 13.8 months, p = 0.08. Three long-term survivors with World Health Organization Grade III tumors were alive with follow-up, ranging from 88-239 months.
Conclusions: High-grade spinal cord primary tumors in children have a poor prognosis. The propensity for neuraxis metastases as a component of progression after RT suggests the need for more aggressive therapy.
Copyright © 2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
Notification: No actual or potential conflicts of interest exist.
Figures
Similar articles
-
Management of pediatric spinal cord astrocytomas: outcomes with adjuvant radiation.Int J Radiat Oncol Biol Phys. 2013 Apr 1;85(5):1307-11. doi: 10.1016/j.ijrobp.2012.11.022. Epub 2013 Feb 20. Int J Radiat Oncol Biol Phys. 2013. PMID: 23433793 Free PMC article.
-
High-grade pediatric spinal cord tumors.Pediatr Neurosurg. 1999 Jan;30(1):1-5. doi: 10.1159/000028751. Pediatr Neurosurg. 1999. PMID: 10202299
-
Long-term outcomes of patients with spinal cord gliomas treated by modern conformal radiation techniques.Int J Radiat Oncol Biol Phys. 2011 Sep 1;81(1):232-8. doi: 10.1016/j.ijrobp.2010.05.009. Epub 2010 Oct 13. Int J Radiat Oncol Biol Phys. 2011. PMID: 20947265
-
Simultaneous integrated boost intensity-modulated radiotherapy in patients with high-grade gliomas.Int J Radiat Oncol Biol Phys. 2010 Oct 1;78(2):390-7. doi: 10.1016/j.ijrobp.2009.08.029. Epub 2010 Jan 25. Int J Radiat Oncol Biol Phys. 2010. PMID: 20097489 Review.
-
Surgical outcomes of pediatric spinal cord astrocytomas: systematic review and meta-analysis.J Neurosurg Pediatr. 2018 Oct;22(4):404-410. doi: 10.3171/2018.4.PEDS17587. Epub 2018 Jul 20. J Neurosurg Pediatr. 2018. PMID: 30028275
Cited by
-
A Systematic Review on the Characteristics, Treatments and Outcomes of the Patients with Primary Spinal Glioblastomas or Gliosarcomas Reported in Literature until March 2015.PLoS One. 2016 Feb 9;11(2):e0148312. doi: 10.1371/journal.pone.0148312. eCollection 2016. PLoS One. 2016. PMID: 26859136 Free PMC article.
-
Prognostic factors and survival in primary malignant astrocytomas of the spinal cord: a population-based analysis from 1973 to 2007.Spine (Phila Pa 1976). 2012 May 20;37(12):E727-35. doi: 10.1097/BRS.0b013e31824584c0. Spine (Phila Pa 1976). 2012. PMID: 22609727 Free PMC article.
-
Management of pediatric spinal cord astrocytomas: outcomes with adjuvant radiation.Int J Radiat Oncol Biol Phys. 2013 Apr 1;85(5):1307-11. doi: 10.1016/j.ijrobp.2012.11.022. Epub 2013 Feb 20. Int J Radiat Oncol Biol Phys. 2013. PMID: 23433793 Free PMC article.
-
Modern treatment of malignant spinal cord astrocytomas: a review article.Med Oncol. 2025 Jul 23;42(8):369. doi: 10.1007/s12032-025-02915-x. Med Oncol. 2025. PMID: 40699374 Review.
-
Recent advances in intradural spinal tumors.Neuro Oncol. 2018 May 18;20(6):729-742. doi: 10.1093/neuonc/nox230. Neuro Oncol. 2018. PMID: 29216380 Free PMC article. Review.
References
-
- Minehan KJ, Brown PD, Scheithauer BW, et al. Prognosis and Treatment of Spinal Cord Astrocytoma. International Journal of Radiation Oncology*Biology*Physics. 2009;73:727–733. - PubMed
-
- Constantini S, Houten J, Miller DC, et al. Intramedullary spinal cord tumors in children under the age of 3 years. J Neurosurg. 1996;85:1036–1043. - PubMed
-
- Bouffet E, Pierre-Kahn A, Marchal J, et al. Prognostic factors in pediatric spinal cord astrocytoma. Cancer. 1998;83:2391–2399. - PubMed
-
- Ciappetta P, Salvati M, Capoccia G, et al. Spinal glioblastomas: report of seven cases and review of the literature. Neurosurgery. 1991;28:302–306. - PubMed
-
- DeSousa AL, Kalsbeck JE, Mealey J, Jr, et al. Intraspinal tumors in children. A review of 81 cases. J Neurosurg. 1979;51:437–445. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
