

Intact PTH combined with the PTH ratio for diagnosis of bone turnover in dialysis patients: a diagnostic test study
- PMID: 20347512
- PMCID: PMC2882243
- DOI: 10.1053/j.ajkd.2009.12.041
Intact PTH combined with the PTH ratio for diagnosis of bone turnover in dialysis patients: a diagnostic test study
Abstract
Background: Determination of parathyroid hormone (PTH) level is the most commonly used surrogate marker for bone turnover in patients with stage 5 chronic kidney disease on dialysis therapy (CKD-5D). The objective of this study is to evaluate the predictive value of various PTH measurements for identifying low or high bone turnover rate.
Study design: Diagnostic test study.
Settings & participants: 141 patients with CKD-5D from 15 US hemodialysis centers.
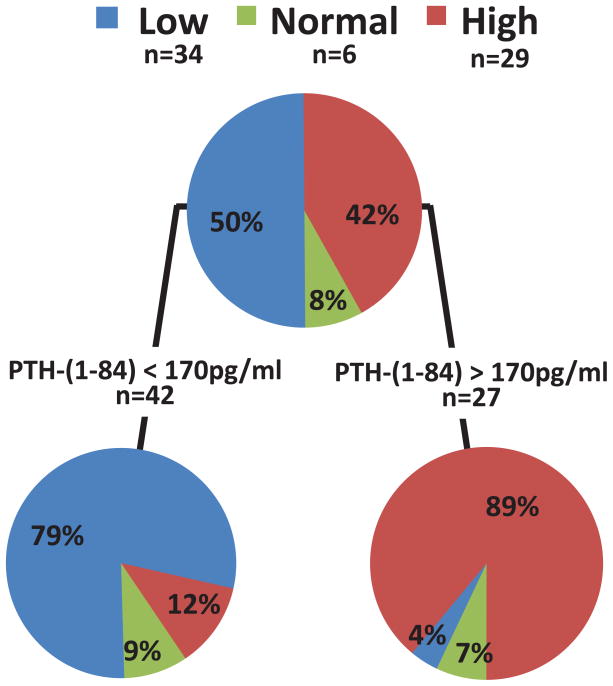
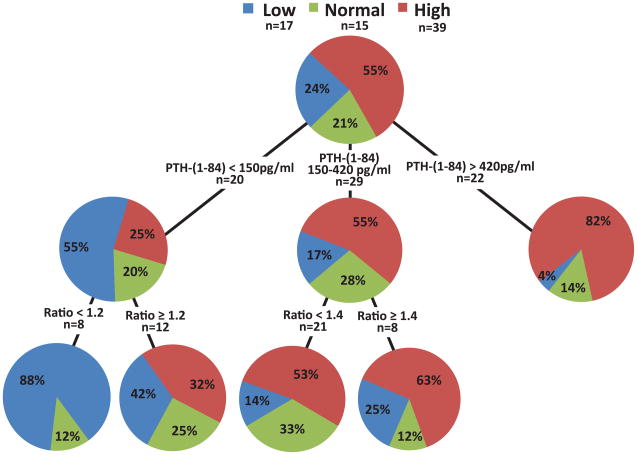
Index tests: Intact PTH, PTH 1-84, and PTH ratio (ratio of level of PTH 1-84 to level of large carboxy-terminal PTH fragments).
Reference test or outcome: Bone turnover determined using bone histomorphometry.
Other measurements: Demographic and treatment-related factors, serum calcium and phosphorus.
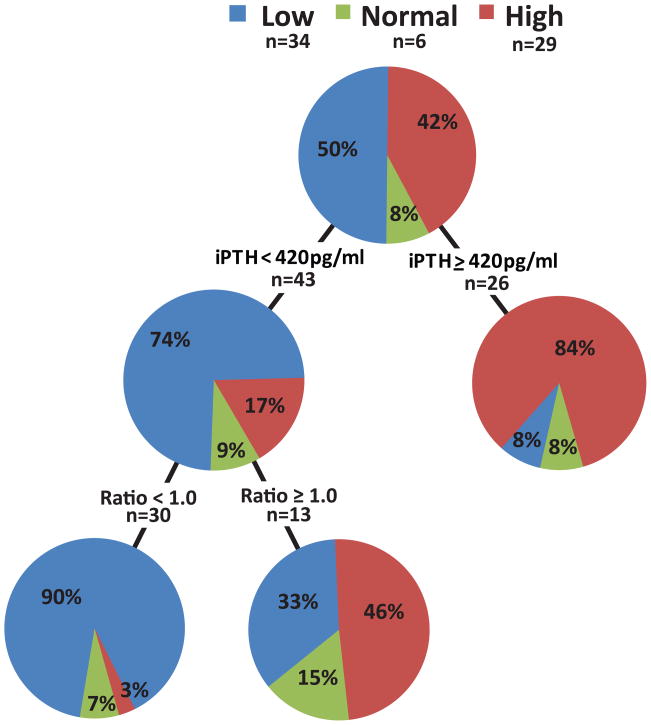
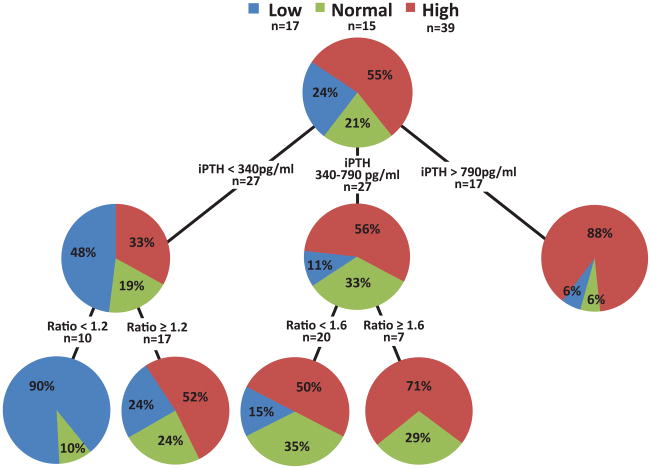
Results: Patients presented histologically with a broad range of bone turnover abnormalities. In white patients with CKD-5D (n = 70), PTH ratio <1.0 added to intact PTH level <420 pg/mL increased the positive predictive value for low bone turnover from 74% to 90%. In black patients (n = 71), adding PTH ratio <1.2 to intact PTH level <340 pg/mL increased the positive predictive value for low bone turnover from 48% to 90%. Adding PTH ratio >1.6 to intact PTH level of 340-790 pg/mL increased the positive predictive value for high bone turnover from 56% to 71%.
Limitations: Because the research protocol called for carefully controlled blood specimen handling, blood drawing and routine specimen handling might be less stringent in clinical practice. By limiting study participation to black and white patients with CKD-5D, we cannot comment on the roles of intact PTH, PTH 1-84, and PTH ratio in other racial/ethnic groups.
Conclusion: In black patients with CKD-5D, the addition of PTH ratio to intact PTH measurements is helpful for diagnosing low and high bone turnover. In white patients with CKD-5D, it aids in the diagnosis of low bone turnover.
Copyright 2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Malluche HH, Monier-Faugere MC. Renal osteodystrophy: what’s in a name? Presentation of a clinically useful new model to interpret bone histologic findings. Clin Nephrol. 2006 Apr;65(4):235–242. - PubMed
-
- Moe S, Drueke T, Cunningham J, et al. Definition, evaluation, and classification of renal osteodystrophy: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO) Kidney Int. 2006 Jun;69(11):1945–1953. - PubMed
-
- Martin KJ, Olgaard K, Coburn JW, et al. Diagnosis, assessment, and treatment of bone turnover abnormalities in renal osteodystrophy. Am J Kidney Dis. 2004 Mar;43(3):558–565. - PubMed
-
- Malluche HH, Monier-Faugere MC. The role of bone biopsy in the management of patients with renal osteodystrophy. J Am Soc Nephrol. 1994;4:1631–1642. - PubMed
-
- Malluche HH, Faugere MC. Atlas of Mineralized Bone Histology. New York: Karger; 1986.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
