

Endogenous cardiotonic steroids and salt-sensitive hypertension
- PMID: 20347967
- PMCID: PMC2933321
- DOI: 10.1016/j.bbadis.2010.03.011
Endogenous cardiotonic steroids and salt-sensitive hypertension
Abstract
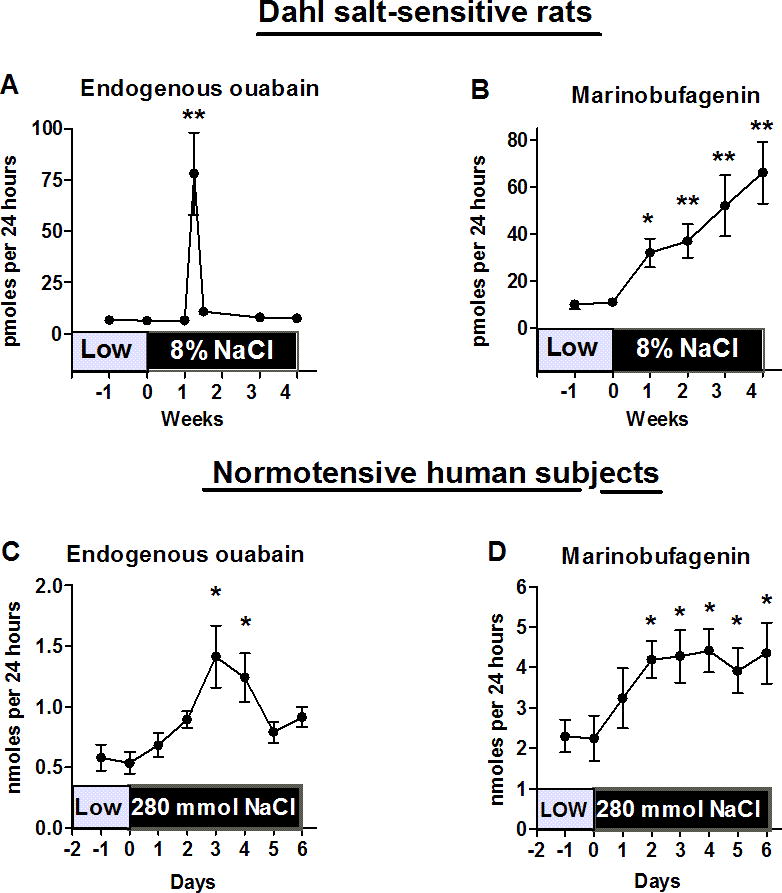
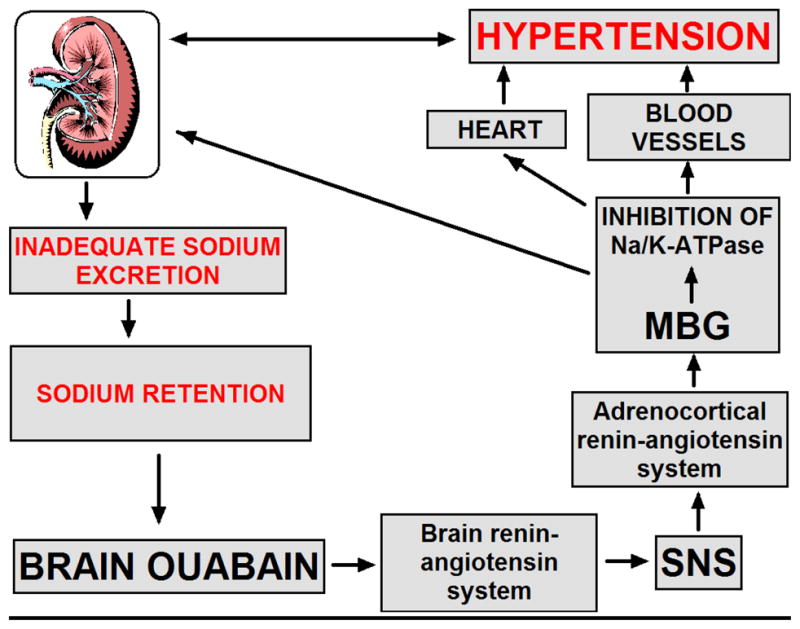
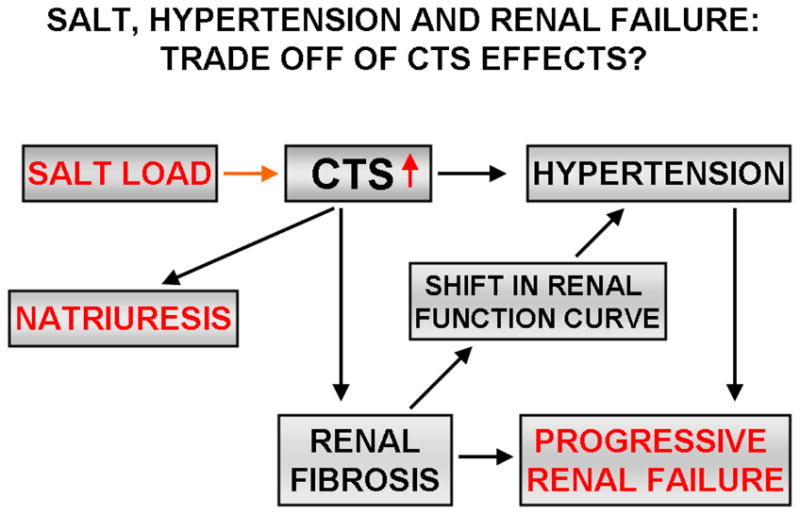
Endogenous cardiotonic steroids (CTS), also called digitalis like factors, have been postulated to play important roles in pathogenesis of hypertension for nearly half of a century. For the past 50 years biomedical scientists have been in quest of an unidentified factor or hormone that both increases blood pressure and renal sodium excretion; this "natriuretic hormone" was, in fact, postulated to interact with the Na/K-ATPase. Recent discoveries have led to the identification of steroid molecules which are present in humans, rodents and amphibians, and which, in a complex manner, interact with each other and with the other systems that regulate renal salt handling and contribute to the salt-sensitivity of blood pressure. Recent findings include the specific identification of endogenous cardenolide (endogenous ouabain) and bufadienolide (marinobufagenin) CTS in humans along with the delineation of mechanisms by which CTS can signal through the Na/K-ATPase. Although CTS were first considered important in the regulation of renal sodium transport and arterial pressure, more recent work implicates these hormones in the central regulation of blood pressure and regulation of cell growth, and development of cardiovascular and renal fibrosis in particular.
Published by Elsevier B.V.
Figures
Similar articles
-
Endogenous cardiotonic steroids: physiology, pharmacology, and novel therapeutic targets.Pharmacol Rev. 2009 Mar;61(1):9-38. doi: 10.1124/pr.108.000711. Pharmacol Rev. 2009. PMID: 19325075 Free PMC article. Review.
-
Cardenolide and bufadienolide ligands of the sodium pump. How they work together in NaCl sensitive hypertension.Front Biosci. 2005 Sep 1;10:2250-6. doi: 10.2741/1694. Front Biosci. 2005. PMID: 15970491 Review.
-
The sodium pump and cardiotonic steroids-induced signal transduction protein kinases and calcium-signaling microdomain in regulation of transporter trafficking.Biochim Biophys Acta. 2010 Dec;1802(12):1237-45. doi: 10.1016/j.bbadis.2010.01.013. Epub 2010 Feb 6. Biochim Biophys Acta. 2010. PMID: 20144708 Free PMC article. Review.
-
Signaling mechanisms that link salt retention to hypertension: endogenous ouabain, the Na(+) pump, the Na(+)/Ca(2+) exchanger and TRPC proteins.Biochim Biophys Acta. 2010 Dec;1802(12):1219-29. doi: 10.1016/j.bbadis.2010.02.011. Epub 2010 Mar 6. Biochim Biophys Acta. 2010. PMID: 20211726 Free PMC article. Review.
-
The pump, the exchanger, and the holy spirit: origins and 40-year evolution of ideas about the ouabain-Na+ pump endocrine system.Am J Physiol Cell Physiol. 2018 Jan 1;314(1):C3-C26. doi: 10.1152/ajpcell.00196.2017. Epub 2017 Nov 7. Am J Physiol Cell Physiol. 2018. PMID: 28971835 Free PMC article. Review.
Cited by
-
Impairment of Na/K-ATPase signaling in renal proximal tubule contributes to Dahl salt-sensitive hypertension.J Biol Chem. 2011 Jul 1;286(26):22806-13. doi: 10.1074/jbc.M111.246249. Epub 2011 May 9. J Biol Chem. 2011. PMID: 21555512 Free PMC article.
-
How safe is unilateral nephrectomy?Hypertension. 2012 Dec;60(6):1383-4. doi: 10.1161/HYPERTENSIONAHA.112.200550. Epub 2012 Oct 15. Hypertension. 2012. PMID: 23071125 Free PMC article. No abstract available.
-
Carbonylation Modification Regulates Na/K-ATPase Signaling and Salt Sensitivity: A Review and a Hypothesis.Front Physiol. 2016 Jun 28;7:256. doi: 10.3389/fphys.2016.00256. eCollection 2016. Front Physiol. 2016. PMID: 27445847 Free PMC article. Review.
-
Molecular mechanisms of experimental salt-sensitive hypertension.J Am Heart Assoc. 2012 Jun;1(3):e002121. doi: 10.1161/JAHA.112.002121. Epub 2012 Jun 22. J Am Heart Assoc. 2012. PMID: 23130148 Free PMC article. No abstract available.
-
The perspective of hypertension and salt intake in Chinese population.Front Public Health. 2023 Feb 17;11:1125608. doi: 10.3389/fpubh.2023.1125608. eCollection 2023. Front Public Health. 2023. PMID: 36875386 Free PMC article. Review.
References
-
- Folkow B. Physiological aspects of primary hypertension. Physiol Rev. 1992;62:347–504. - PubMed
-
- DeWardener HE, Clarkson EM. Concept of natriuretic hormone. Physiol Rev. 1985;65:658–759. - PubMed
-
- Dahl LK, Knudsen KD, Iwai J. Humoral transmission of hypertension: Evidence from parabiosis. Circ Res. 1969;24(5Suppl):21–33. - PubMed
-
- Blaustein MP. Sodium ions, calcium ions, blood pressure regulation and hypertension: A reassessment and a hypothesis. Am J Physiol. 1977;232:C167–C173. - PubMed
-
- Haddy FJ, Overbeck HW. The role of humoral agents in volume expanded hypertension. Life Sci. 1976;19:935–947. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
