

Antenatal steroids in preterm labour for the prevention of neonatal deaths due to complications of preterm birth
- PMID: 20348115
- PMCID: PMC2845868
- DOI: 10.1093/ije/dyq029
Antenatal steroids in preterm labour for the prevention of neonatal deaths due to complications of preterm birth
Abstract
Background: In high-income countries, administration of antenatal steroids is standard care for women with anticipated preterm labour. However, although >1 million deaths due to preterm birth occur annually, antenatal steroids are not routine practice in low-income countries where most of these deaths occur.
Objectives: To review the evidence for and estimate the effect on cause-specific neonatal mortality of administration of antenatal steroids to women with anticipated preterm labour, with additional analysis for the effect in low- and middle-income countries.
Methods: We conducted systematic reviews using standardized abstraction forms. Quality of evidence was assessed using an adapted GRADE approach. Existing meta-analyses were reviewed for relevance to low/middle-income countries, and new meta-analysis was performed.
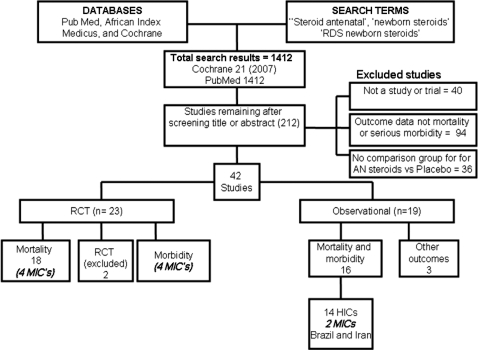
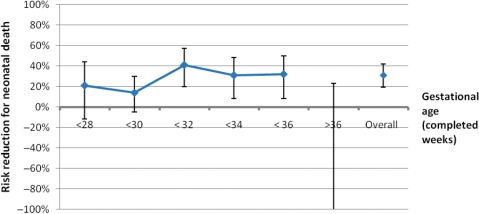
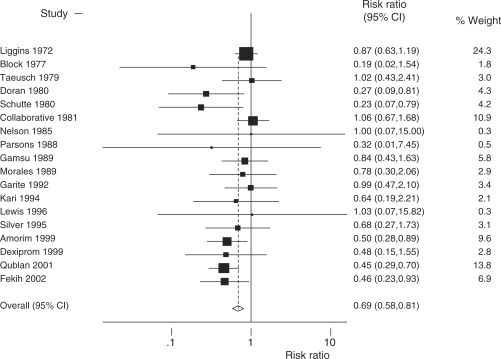
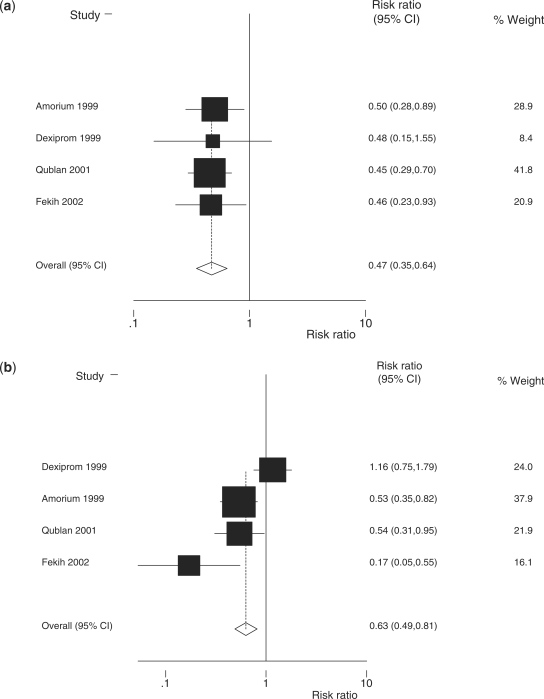
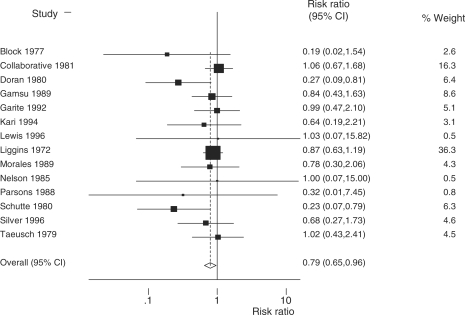
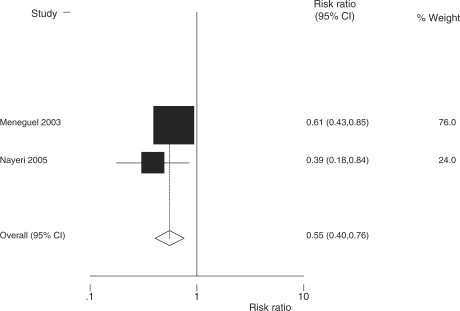
Results: We identified 44 studies, including 18 randomised control trials (RCTs) (14 in high-income countries) in a Cochrane meta-analysis, which suggested that antenatal steroids decrease neonatal mortality among preterm infants (<36 weeks gestation) by 31% [relative risk (RR) = 0.69; 95% confidence interval (CI) 0.58-0.81]. Our new meta-analysis of four RCTs from middle-income countries suggests 53% mortality reduction (RR = 0.47; 95% CI 0.35-0.64) and 37% morbidity reduction (RR = 0.63; 95% CI 0.49-0.81). Observational study mortality data were consistent. The control group in these equivalent studies was routine care (ventilation and, in many cases, surfactant). In low-income countries, many preterm babies currently receive little or no medical care. It is plausible that antenatal steroids may be of even greater effect when tested in these settings.
Conclusions: Based on high-grade evidence, antenatal steroid therapy is very effective in preventing neonatal mortality and morbidity, yet remains at low coverage in low/middle-income countries. If fully scaled up, this intervention could save up to 500 000 neonatal lives annually.
Figures
References
-
- Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths: when? Where? Why? Lancet. 2005;365:891–900. - PubMed
-
- Avery ME, Mead J. Surface properties in relation to atelectasis and hyaline membrane disease. Am J Dis Child. 1959;97:517–23. - PubMed
-
- Whitsett JA, Pryhuber GS, Rice WR, Warner BB, Wert SE. Acute respiratory disorders. In: Avery GB, Fletcher MA, MacDonald MG, editors. Neonatology: Pathophysiology and Management of the Newborn. 4th. Philadelphia: J.B. Lippincott Company; 1994. pp. 429–52.
-
- Hjalmarson O. Epidemiology and classification of acute neonatal respiratory disorders. A prospective study. Acta Paediatr Scand. 1981;70:773–83. - PubMed
-
- Farrell PM, Avery ME. Hyaline membrane disease. Am Rev Respir Dis. 1975;111:657–85. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
