

17-alpha-hydroxyprogesterone caproate for the prevention of preterm birth in women with prior preterm birth and a short cervical length
- PMID: 20350641
- PMCID: PMC2855838
- DOI: 10.1016/j.ajog.2010.02.019
17-alpha-hydroxyprogesterone caproate for the prevention of preterm birth in women with prior preterm birth and a short cervical length
Abstract
Objective: We sought to evaluate 17-alpha-hydroxyprogesterone caproate (17P) for prevention of preterm birth (PTB) in women with prior spontaneous PTB (SPTB) and cervical length (CL) <25 mm.
Study design: We conducted planned secondary analysis of the Eunice Kennedy Shriver National Institute of Child Health and Human Development-sponsored randomized trial evaluating cerclage for women with singleton gestations, prior SPTB (17-33 6/7 weeks), and CL <25 mm between 16-22 6/7 weeks. Women were stratified at randomization to intent to use or not use 17P. The effect of 17P was analyzed separately for cerclage and no-cerclage groups. Primary outcome was PTB <35 weeks.
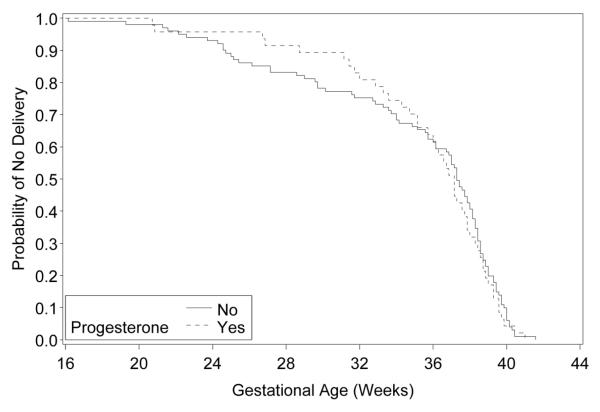
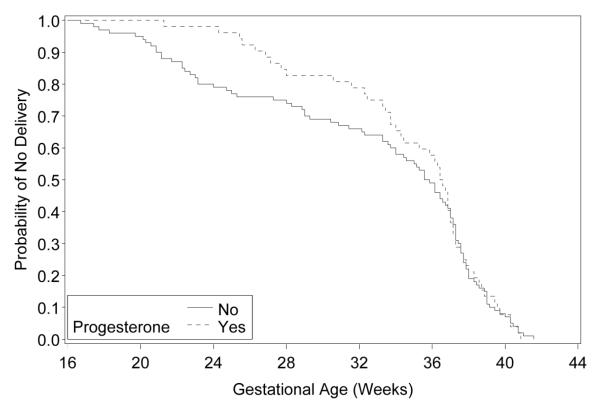
Results: In 300 women, 17P had no effect on PTB <35 weeks in either cerclage (P = .64) or no-cerclage (P = .51) groups. Only PTB <24 weeks (odds ratio, 0.08) and perinatal death (odds ratio, 0.14) were significantly lower for those with 17P in the no-cerclage group.
Conclusion: 17P had no additional benefit for prevention of PTB in women who had prior SPTB and got ultrasound-indicated cerclage for CL <25 mm. In women who did not get cerclage, 17P reduced previable birth and perinatal mortality.
Copyright 2010 Mosby, Inc. All rights reserved.
Figures
References
-
- Iams JD, Goldenberg RL, Meis PJ, Mercer BM, Moawad A, Das A, et al. The length of the cervix and the risk of spontaneous premature delivery. NEJM. 1996;334(9):567–72. - PubMed
-
- Mercer BM, Goldenberg RL, Moawad AH, Meis PJ, Iams JD, das AF, et al. The preterm prediction study: effect of gestational age and cause of preterm birth on subsequent obstetric outcome. Am J Obstet Gynecol. 1999;181:1216–21. - PubMed
-
- Rust OA, Atlas RO, Reed J, van Gaalen J, Balducci J. Revisiting the short cervix detected by transvaginal ultrasound in the second trimester: Why cerclage therapy may not help. Am J Obstet Gynecol. 2001;185:1098–105. - PubMed
-
- Althuisius SM, Dekker GA, Hummel P, Bekedam DJ, van Geijn HP. Final results of the cervical incompetence prevention randomized cerclage trial (CIPRACT): Therapeutic cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol. 2001;185:1106–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
