

Patterns and correlates of adjuvant radiotherapy receipt after lumpectomy and after mastectomy for breast cancer
- PMID: 20351324
- PMCID: PMC2881720
- DOI: 10.1200/JCO.2009.26.8433
Patterns and correlates of adjuvant radiotherapy receipt after lumpectomy and after mastectomy for breast cancer
Abstract
Purpose: To use patient self-report to provide more valid estimates of whether radiotherapy (RT) is underutilized than possible with registry data, as well as to evaluate for disparities and the influence of preferences and provider interactions.
Methods: We considered 2,260 survey respondents who had nonmetastatic breast cancer, were age 20 to 79 years, were diagnosed between July 2005 and February 2007 in Detroit and Los Angeles, and reported to Surveillance, Epidemiology and End Results (SEER) registries (72% response rate). Survey responses were merged with SEER data. We assessed rates and correlates of RT receipt among all patients with invasive cancer receiving breast-conserving surgery (BCS) and among patients undergoing mastectomy with indications for RT (ie, positive lymph nodes or T3-4 tumors).
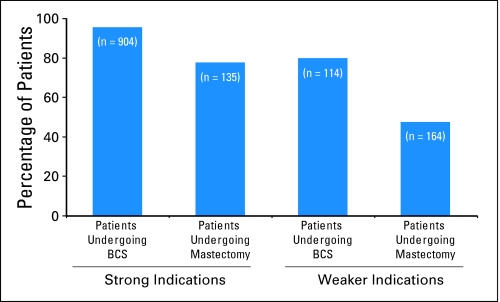
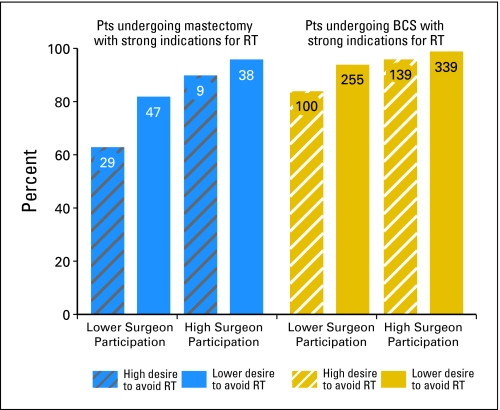
Results: Among 904 patients undergoing BCS with strong indications for RT, 95.4% received RT, and 77.6% received RT among the 135 patients undergoing mastectomy with strong indications (P < .001). Among 114 patients undergoing BCS with weaker indications (ie, elderly) for RT, 80.0% received treatment, and 47.5% received RT among the 164 patients undergoing mastectomy with weaker indications (T1N1, T2N1, or T3N0 disease; P < .001). On multivariate analysis, surgery type (P < .001), indication strength (P < .001), age (P = .005), comorbidity (P < .001), income (P = .03), patient desire to avoid RT (P < .001), level of surgeon involvement in decision to have radiation (P < .001), and SEER site (P < .001) were significantly associated with likelihood of RT receipt.
Conclusion: RT receipt was consistently high across sociodemographic subgroups after BCS but was lower after mastectomy, even among patients with strong indications for treatment, in whom clinical benefit is similar. Surgeon involvement had a strong influence on RT receipt.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Similar articles
-
Breast cancer among the oldest old: tumor characteristics, treatment choices, and survival.J Clin Oncol. 2010 Apr 20;28(12):2038-45. doi: 10.1200/JCO.2009.25.9796. Epub 2010 Mar 22. J Clin Oncol. 2010. PMID: 20308658 Free PMC article.
-
Does it matter where you go for breast surgery?: attending surgeon's influence on variation in receipt of mastectomy for breast cancer.Med Care. 2010 Oct;48(10):892-9. doi: 10.1097/MLR.0b013e3181ef97df. Med Care. 2010. PMID: 20808256 Free PMC article.
-
Patterns and correlates of local therapy for women with ductal carcinoma-in-situ.J Clin Oncol. 2005 May 1;23(13):3001-7. doi: 10.1200/JCO.2005.04.028. J Clin Oncol. 2005. PMID: 15860856 Free PMC article.
-
Decision involvement and receipt of mastectomy among racially and ethnically diverse breast cancer patients.J Natl Cancer Inst. 2009 Oct 7;101(19):1337-47. doi: 10.1093/jnci/djp271. Epub 2009 Aug 31. J Natl Cancer Inst. 2009. PMID: 19720966 Free PMC article.
-
Socioeconomic status and breast cancer treatment.Breast Cancer Res Treat. 2018 Jan;167(1):1-8. doi: 10.1007/s10549-017-4490-3. Epub 2017 Sep 7. Breast Cancer Res Treat. 2018. PMID: 28884392 Free PMC article. Review.
Cited by
-
Narrowing Racial Gaps in Breast Cancer: Factors Affecting Probability of Adjuvant Radiation Therapy.Adv Radiat Oncol. 2019 Aug 16;5(1):17-26. doi: 10.1016/j.adro.2019.07.014. eCollection 2020 Jan-Feb. Adv Radiat Oncol. 2019. PMID: 32051886 Free PMC article.
-
Considerations for observational research using large data sets in radiation oncology.Int J Radiat Oncol Biol Phys. 2014 Sep 1;90(1):11-24. doi: 10.1016/j.ijrobp.2014.05.013. Int J Radiat Oncol Biol Phys. 2014. PMID: 25195986 Free PMC article. Review.
-
Trends in the Application of Postmastectomy Radiotherapy for Breast Cancer With 1 to 3 Positive Axillary Nodes and Tumors ≤5 cm in the Modern Treatment Era: A Retrospective Korean Breast Cancer Society Report.Medicine (Baltimore). 2016 May;95(19):e3592. doi: 10.1097/MD.0000000000003592. Medicine (Baltimore). 2016. PMID: 27175662 Free PMC article.
-
Breast Cancer Treatment Following Health Reform: Evidence From Massachusetts.Med Care Res Rev. 2022 Jun;79(3):371-381. doi: 10.1177/10775587211042532. Epub 2021 Sep 1. Med Care Res Rev. 2022. PMID: 34467806 Free PMC article.
-
Postmastectomy radiation therapy: an overview for the practicing surgeon.ISRN Surg. 2013 Sep 11;2013:212979. doi: 10.1155/2013/212979. ISRN Surg. 2013. PMID: 24109522 Free PMC article. Review.
References
-
- Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;366:2087–2106. - PubMed
-
- Lazovich DA, White E, Thomas DB, et al. Underutilization of breast-conserving surgery and radiation therapy among women with stage I or II breast cancer. JAMA. 1991;266:3433–3438. - PubMed
-
- Farrow DC, Hunt WC, Samet JM. Geographic variation in the treatment of localized breast cancer. N Engl J Med. 1992;326:1097–1101. - PubMed
-
- Nattinger AB, Hoffmann RG, Kneusel RT, et al. Relation between appropriateness of primary therapy for early-stage breast carcinoma and increased use of breast-conserving surgery. Lancet. 2000;356:1148–1153. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
