

Amblyopia in astigmatic infants and toddlers
- PMID: 20351602
- PMCID: PMC2886599
- DOI: 10.1097/OPX.0b013e3181d951c8
Amblyopia in astigmatic infants and toddlers
Abstract
Purpose: To determine whether reduced astigmatism-corrected acuity for vertical (V) and/or horizontal (H) gratings and/or meridional amblyopia (MA) are present before 3 years of age in children who have with-the-rule astigmatism.
Methods: Subjects were 448 children, 6 months through 2 years of age with no known ocular abnormalities other than with-the-rule astigmatism, who were recruited through Women, Infants and Children clinics on the Tohono O'odham reservation. Children were classified as non-astigmats (< or =2.00 diopters) or astigmats (>2.00 diopters) based on right eye non-cycloplegic autorefraction measurements (Welch Allyn SureSight). Right eye astigmatism-corrected grating acuity for V and H stimuli was measured using the Teller Acuity Card procedure while children wore cross-cylinder lenses to correct their astigmatism or plano lenses if they had no astigmatism.
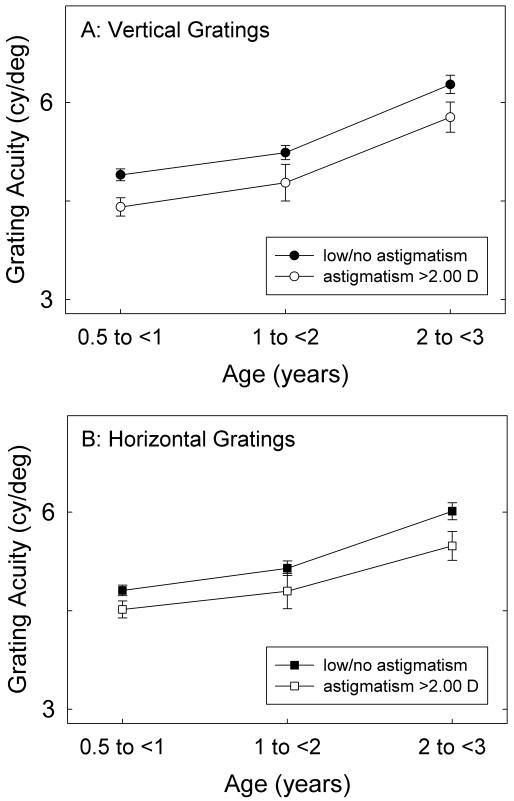
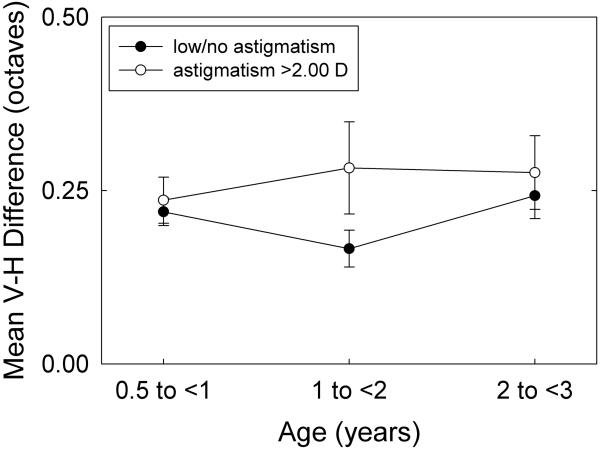
Results: Astigmatism-corrected acuity for both V and H gratings was significantly poorer in the astigmats than in the non-astigmats, and the reduction in acuity for astigmats was present for children in all three age groups examined (6 months to <1 year, 1 to <2 years, and 2 to <3 years). There was no significant difference in V-H grating acuity (no evidence of MA) for the astigmatic group as a whole, or when data were analyzed for each age group.
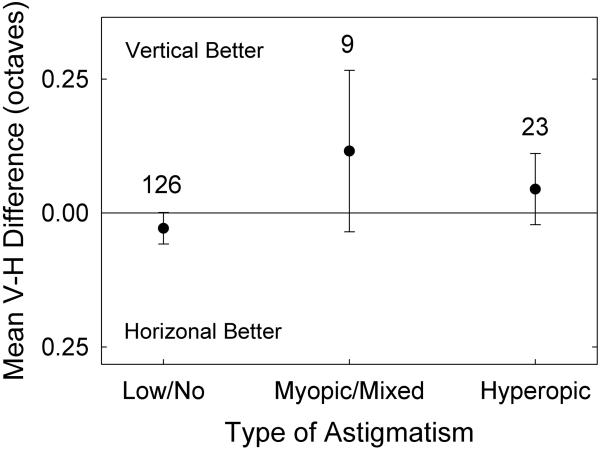
Conclusions: Even in the youngest age group, astigmats tested with astigmatism correction showed reduced acuity for both V and H gratings, which suggests that astigmatism is having a negative influence on visual development. We found no evidence of orientation-related differences in astigmatism-corrected grating acuity, indicating either that MA does not develop before 3 years of age, or that most of the astigmatic children had a type of astigmatism, i.e., hyperopic, that has proven to be less likely than myopic or mixed astigmatism to result in MA.
Figures
Similar articles
-
Optical treatment reduces amblyopia in astigmatic children who receive spectacles before kindergarten.Ophthalmology. 2009 May;116(5):1002-8. doi: 10.1016/j.ophtha.2008.11.013. Epub 2009 Feb 20. Ophthalmology. 2009. PMID: 19232733
-
Amblyopia in astigmatic preschool children.Vision Res. 2003 Apr;43(9):1081-90. doi: 10.1016/s0042-6989(03)00014-2. Vision Res. 2003. PMID: 12676249
-
Optical treatment of amblyopia in astigmatic children: the sensitive period for successful treatment.Ophthalmology. 2007 Dec;114(12):2293-301. doi: 10.1016/j.ophtha.2007.03.021. Ophthalmology. 2007. PMID: 18054643
-
Changes in visual function following optical treatment of astigmatism-related amblyopia.Vision Res. 2008 Mar;48(6):773-87. doi: 10.1016/j.visres.2007.12.007. Epub 2008 Feb 7. Vision Res. 2008. PMID: 18261760 Free PMC article.
-
Development and treatment of astigmatism-related amblyopia.Optom Vis Sci. 2009 Jun;86(6):634-9. doi: 10.1097/OPX.0b013e3181a6165f. Optom Vis Sci. 2009. PMID: 19430327 Free PMC article. Review.
Cited by
-
Genome-wide meta-analysis of five Asian cohorts identifies PDGFRA as a susceptibility locus for corneal astigmatism.PLoS Genet. 2011 Dec;7(12):e1002402. doi: 10.1371/journal.pgen.1002402. Epub 2011 Dec 1. PLoS Genet. 2011. PMID: 22144915 Free PMC article.
-
Evaluation of the Prevalence of Refractive Defects and Ocular Function in a Group of 1518 Children Aged 8 Years in Northwestern Poland-A Retrospective Study.J Clin Med. 2023 Apr 14;12(8):2880. doi: 10.3390/jcm12082880. J Clin Med. 2023. PMID: 37109217 Free PMC article.
-
Age norms for grating acuity and contrast sensitivity measured by Lea tests in the first three years of life.Int J Ophthalmol. 2017 Jul 18;10(7):1150-1153. doi: 10.18240/ijo.2017.07.20. eCollection 2017. Int J Ophthalmol. 2017. PMID: 28730121 Free PMC article.
-
The Performance of Spot Photoscreener in 6 to 10 Weeks Infants in China: A Cross-Sectional Study.J Ophthalmol. 2024 May 11;2024:8817530. doi: 10.1155/2024/8817530. eCollection 2024. J Ophthalmol. 2024. PMID: 38765182 Free PMC article.
-
Higher-order aberrations and best-corrected visual acuity in Native American children with a high prevalence of astigmatism.J AAPOS. 2015 Aug;19(4):352-7.e1. doi: 10.1016/j.jaapos.2015.05.004. Epub 2015 Jul 31. J AAPOS. 2015. PMID: 26239206 Free PMC article.
References
-
- Atkinson J, Braddick O, Robier B, Anker S, Ehrlich D, King J, Watson P, Moore A. Two infant vision screening programmes: prediction and prevention of strabismus and amblyopia from photo- and videorefractive screening. Eye. 1996;10(Pt 2):189–98. - PubMed
-
- Cobb SR, MacDonald CF. Resolution acuity in astigmats: evidence for a critical period in the human visual system. Br J Physiol Opt. 1978;32:38–49. - PubMed
-
- Dobson V, Miller JM, Harvey EM, Mohan KM. Amblyopia in astigmatic preschool children. Vision Res. 2003;43:1081–90. - PubMed
-
- Freeman RD. Contrast sensitivity in meridional amblyopia. Invest Ophthalmol. 1975;14:78–81. - PubMed
-
- Freeman RD, Mitchell DE, Millodot M. A neural effect of partial visual deprivation in humans. Science. 1972;175:1384–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
